A man in his 40s w/ untreated HIV presented w/ severe palmoplantar keratoderma, nail dystrophy, dactylitis, & numerous well-demarcated dull-red hyperkeratotic to cone-shaped plaques involving the extremities, scalp, ears, & face. Labs showed profound immunosuppression (CD4 count 5 cells/µL), pancytopenia, & -ve syphilis serologies.
What’s your DDx❔
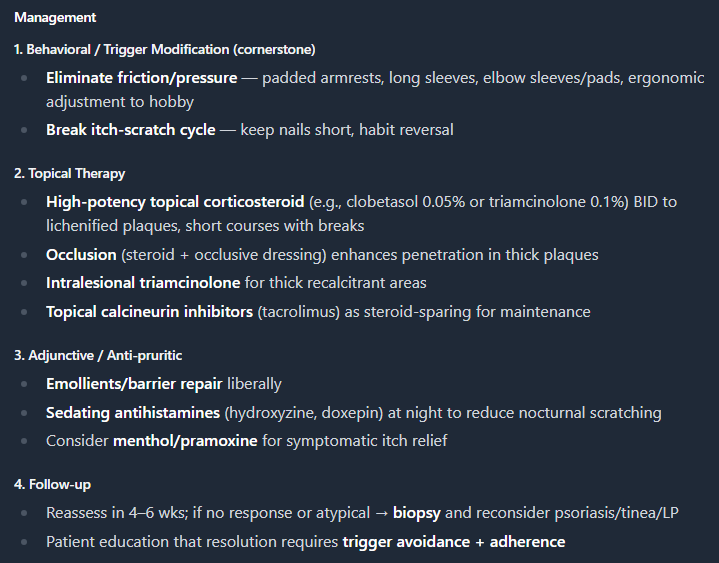
Diagnosis: Frictional lichenification (lichen simplex chronicus) 2/2 chronic mechanical pressure & repetitive friction from chair armrests.
Further hx revealed that the eruption waxed & waned w/ the frequency of the patient's seated hobby of gaming & the condition of the chair armrests. He routinely rested & rubbed his forearms against worn, inadequately padded armrests for prolonged periods, often with significant sweating, producing repetitive friction at the exact sites of involvement.
The morphology and distribution of the lesions corresponded closely to these contact points, supporting a friction-induced dermatosis. Similar activity-related dermatoses have been described in association w/ prolonged gaming and other repetitive recreational activities, including friction-induced eccrine hidradenitis & controller-related hyperkeratotic lesions. In this case, chronic pressure, friction, and moisture led to localized lichenification of the elbows & dorsal forearms.
Mx consisted of behavioral & ergonomic modifications, including improved armrest padding and minimizing repetitive friction, along w/ topical corticosteroids & emollients. These measures resulted in progressive symptomatic improvement and resolution of the lichenified plaques.
<GPT-5.5 & Claude Opus 4.8>
A man in his 30s presented w/ a chronic pruritic eruption involving the B/L elbows & dorsal forearms. Symptoms were mildly tender & worsened w/ prolonged periods of a repetitive seated hobby that involved resting his forearms on chair armrests. He denied new topical exposures, outdoor triggers, or a personal hx of AD, psoriasis, or other chronic dermatoses.
What’s the diagnosis❔
Diagnosis: Frictional lichenification (lichen simplex chronicus) 2/2 chronic mechanical pressure & repetitive friction from chair armrests.
Further hx revealed that the eruption waxed & waned w/ the frequency of the patient's seated hobby of gaming & the condition of the chair armrests. He routinely rested & rubbed his forearms against worn, inadequately padded armrests for prolonged periods, often with significant sweating, producing repetitive friction at the exact sites of involvement.
The morphology and distribution of the lesions corresponded closely to these contact points, supporting a friction-induced dermatosis. Similar activity-related dermatoses have been described in association w/ prolonged gaming and other repetitive recreational activities, including friction-induced eccrine hidradenitis & controller-related hyperkeratotic lesions. In this case, chronic pressure, friction, and moisture led to localized lichenification of the elbows & dorsal forearms.
Mx consisted of behavioral & ergonomic modifications, including improved armrest padding and minimizing repetitive friction, along w/ topical corticosteroids & emollients. These measures resulted in progressive symptomatic improvement and resolution of the lichenified plaques.
<GPT-5.5 & Claude Opus 4.8>
Diagnosis: Frictional lichenification (lichen simplex chronicus) 2/2 chronic mechanical pressure & repetitive friction from chair armrests.
Further hx revealed that the eruption waxed & waned w/ the frequency of the patient's seated hobby of gaming & the condition of the chair armrests. He routinely rested & rubbed his forearms against worn, inadequately padded armrests for prolonged periods, often with significant sweating, producing repetitive friction at the exact sites of involvement.
The morphology and distribution of the lesions corresponded closely to these contact points, supporting a friction-induced dermatosis. Similar activity-related dermatoses have been described in association w/ prolonged gaming and other repetitive recreational activities, including friction-induced eccrine hidradenitis & controller-related hyperkeratotic lesions. In this case, chronic pressure, friction, and moisture led to localized lichenification of the elbows & dorsal forearms.
Mx consisted of behavioral & ergonomic modifications, including improved armrest padding and minimizing repetitive friction, along w/ topical corticosteroids & emollients. These measures resulted in progressive symptomatic improvement and resolution of the lichenified plaques.
<GPT-5.5 & Claude Opus 4.8>
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
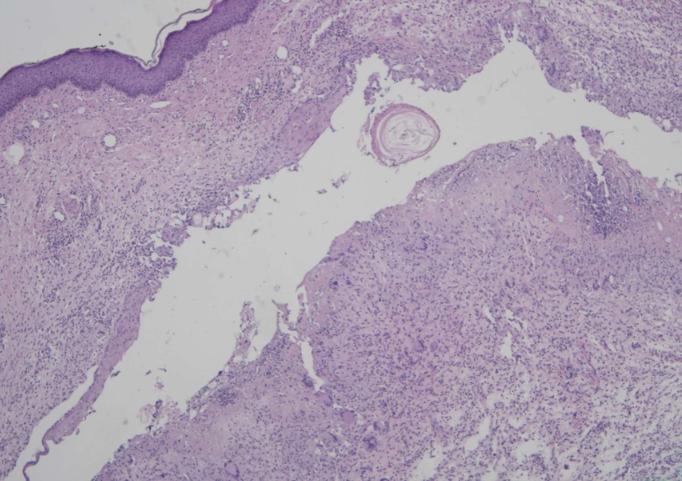
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
An adolescent girl w/ no significant PMHx presented w/ a 3-mo hx of a lesion on the right posterior arm, first noted after the abrupt onset of localized burning pain. She denied preceding trauma, insect bites, drainage, relevant travel, or environmental exposures. Prior tx w/ topical clindamycin & mupirocin was ineffective.
O/E: two adjacent atrophic plaques w/ surrounding erythema on the right posterior arm.
Dermoscopy demonstrated prominent looped vessels over a yellow-white globular background.
What’s your DDx❔
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
An adolescent girl w/ no significant PMHx presented w/ a 3-mo hx of a lesion on the right posterior arm, first noted after the abrupt onset of localized burning pain. She denied preceding trauma, insect bites, drainage, relevant travel, or environmental exposures. Prior tx w/ topical clindamycin & mupirocin was ineffective.
O/E: two adjacent atrophic plaques w/ surrounding erythema on the right posterior arm.
Dermoscopy demonstrated prominent looped vessels over a yellow-white globular background.
What’s your DDx❔
Diagnosis: Cutaneous Mycobacterium abscessus infection associated with a ruptured epidermal inclusion cyst (EIC).
A punch bx showed suppurative granulomatous dermatitis w/in a scar, raising concern for an infectious process despite -ve PAS, Gram, Fite, & auramine-rhodamine stains. Repeat excisional bx demonstrated a ruptured EIC w/ surrounding granulomatous inflammation. Although bacterial & fungal cultures were -ve, AFB tissue culture grew M. abscessus, establishing the dx of a cutaneous rapidly growing nontuberculous mycobacterial (NTM) infection coexisting with a ruptured EIC.
The lesion was completely excised, & susceptibility-guided therapy w/ azithromycin was administered for 3 mos (macrolide-sensitive, tetracycline-resistant isolate), resulting in complete clinical resolution.
DDx: deep fungal infection (sporotrichosis, phaeohyphomycosis, blastomycosis), cutaneous leishmaniasis, foreign-body granuloma, granuloma annulare, morphea / localized scleroderma, atrophoderma, cutaneous sarcoidosis, dermatofibroma.
🔑 Chronic, tx-refractory cutaneous lesions w/ granulomatous inflammation should prompt consideration of NTM infection, even when special stains are -ve, as cx may be required for definitive dx.
COVID-19–associated secondary hemophagocytic lymphohistiocytosis (HLH) presenting as a severe acute mucocutaneous inflammatory syndrome.
A recent COVID-19 infection triggered a hyperinflammatory syndrome characterized by fever, diffuse morbilliform eruption, hemorrhagic mucositis, conjunctivitis, pseudochilblains w/ livedo racemosa, cervical LAD, & marked orofacial edema progressing to respiratory compromise. The DDx at that time was RIME, MIS-A, DRESS, SJS/TEN, adult-onset Still disease, & COVID-associated HLH.
Labs demonstrated pancytopenia, hyperferritinemia, hypertriglyceridemia, elevated soluble IL-2 receptor levels, and decreased NK-cell activity. Bone marrow bx revealed hemophagocytosis and prominent emperipolesis (see infra). The patient met 7 of 8 HLH-2004 criteria, confirming secondary HLH. The mucocutaneous findings preceded neurologic deterioration & likely represented an early manifestation of systemic immune dysregulation.
Treatment with etoposide led to gradual clinical recovery over 6 months. The presence of emperipolesis indicates severe immune activation & expands the spectrum of marrow findings reported in COVID-19–associated HLH.
A previously healthy woman in her 20s presented w/ 1-wk of rapidly progressive fever, rash, & severe orofacial edema requiring intubation. She reported a viral prodrome 2 weeks earlier, and SARS-CoV-2 IgM was +ve, consistent w/ recent COVID-19 infection.
O/E: cervical LAD, marked periorificial edema, diffuse morbilliform eruption of the trunk, hemorrhagic oral erosions, B/L conjunctivitis, mild hand arthralgia/synovitis, & acral pseudochilblains w/ livedo racemosa of the palms & soles.
What’s your DDx❔