Will be the largest antigen-specific atlas of humoral immunity yet-constructed with >16K cancer and aging serum samples.
Thank you to @CancerGrand & @casanova_lab for supporting and taking a chance on this.
Congrats to Ludwig Oxford Director Xin Lu and Chi Van Dang, CEO & scientific director of the Ludwig Institute for Cancer Research, who’ve received a Cancer Grand Challenges award as members of the ATLAS team to take on the challenge of “Cancer Avoidance”. https://t.co/GddhZXoGxi
Impacts of antigenic first sin on antiviral antibodies? Well established; observed again here.
Impacts of antigenic first sin on autoantibodies? Entirely unexplored. Imagine our very first immune mistakes lead to a lifetime of health impacts…
New data from David Ho's lab showing that while adults & kids have ~equal antibody responses to XFG & NB.1.8.1, children have essentially no neutralizing antibodies to BA.3.2.
This seems to largely solve the BA.3.2 + kids mystery. 1/14
^I still like the “can’t beat evolution” re: danger of potential off-world pathogens; ie how could a bug on Mars be better at killing you than one evolved to do that here? But horizontal transfer within earth pathogens / smallpox resurrection - that scares me….
It’s nearly impossible to beat viral evolution. But simple horizontal transfer of naturally evolved traits is trivial to try, can create surprising results.
Sometimes all it takes is swapping in that interesting new pangolin RBD, maybe a well placed furin cleavage site…
Pretending like someone with an AI model and some gene synthesis is anything close in threat scale to the horrible diseases that we have spent centuries beating back serves more to market AI tools than provide a sober realistic assessment of threats
We often think of tumor antigens as mere passengers. But the frequency of some suggests beneficial selection and perhaps more “evasion mechanism” than “antigen”…
Tumors like decorating themselves with PD-L1 for a reason. Could it be the same for MAGEA3 et al?
I've been hand-waving a lot about how under-appreciated cancer-testis antigens are as an alt target space for personalized immunotherapies.
Starting to put numbers on potential impact, eg how many patients have high expression of 1+ CTA.
first attempt: ~1/3 of all cancers
While we ran these arrays - something special I’d missed.
Most autoantibodies are private. Categorical enrichments happen. Known! (Fig 3I).
But private autoabs within an ontology … another layer entirely (Fig 3J).
Suggests (mechanistic?) individuality beyond shared abs!
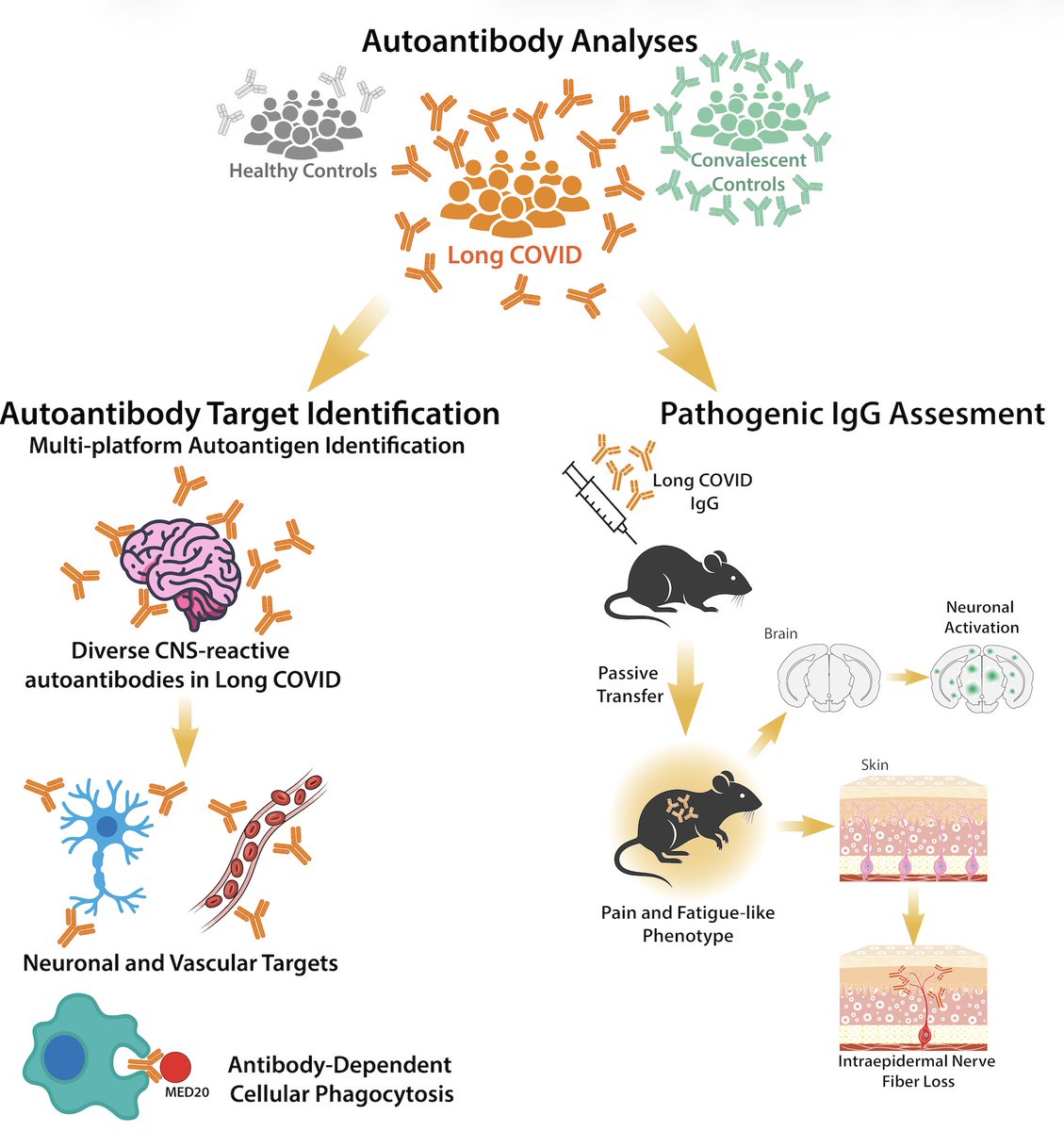
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
@dina_said_that A good question but I honestly would not know. I think most autoimmune conditions that matter remain undiscovered - and that bedridden patients could have something like the test you describe, or something currently hard to find that there currently is not a test for…
Did the daratumumab *just* destroy the myeloma - or did it *also* knock out a T-cell suppressing autoantibody? Daratumumab depletes long-lived plasma cells via CD38 & potentially-harmful immune-altering autoantibodies - not just the cancer! @casanova_lab
Sometimes cancer treatments are subject to hype, but here’s an advance that’s been understated:
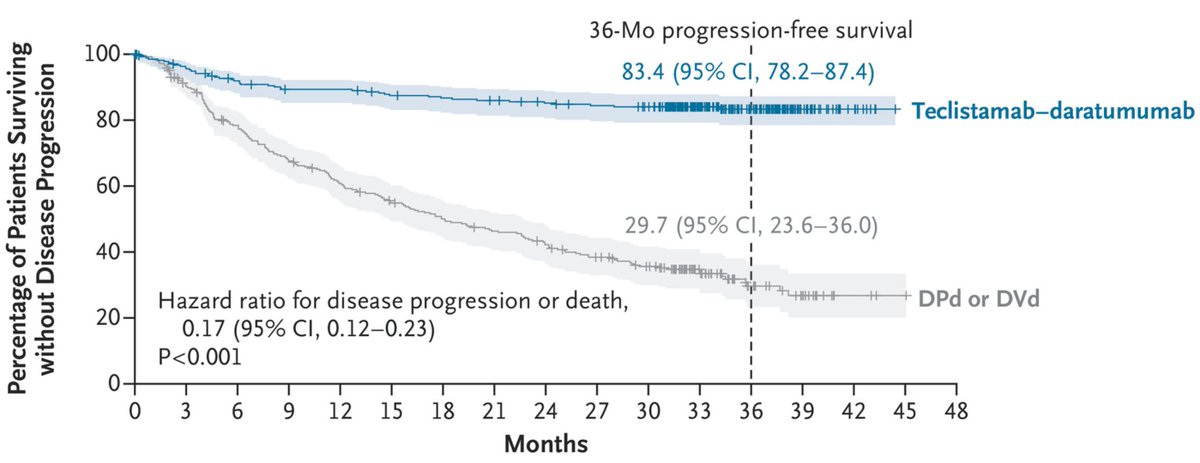
Combining a T-cell engager antibody with daratumumab allowed >80% of people with relapsed or refractory multiple myeloma to go years without progression. Might be *permanent* control
Thrilled to share our new preprint: "AEGIS reveals epitope- and clone-resolved convergence of CNS B and T cell autoreactivity in ROHHAD." Important implications for mechanistically understanding autoimmunity! Massive team effort (attributions at end).
https://t.co/hhciZUn3f0
@SanjayNadaraja@ruth_hook_ Again - yes. Strength training is best current intervention even if I’m right here. But you might also need something like a tolerance vaccine to truly eliminate the problem. Immunity can cause weird permanent effects, most of which we don’t yet understand…
@SanjayNadaraja@ruth_hook_ For sure - I am not 'disagreeing' - strength training improves immune tolerance too. I also just don't think it's 'normal' for old ladies bones to start breaking more than men's irrespective of diet and lifestyle.
@anna_reise87030@32Sfc46582 I’m hopeful that we can find a simpler mechanism autoantibody that can be treated easier. There’s great new work on antibody-caused B12 deficiency. Maybe something like that can be found and then there’s a simpler fix in a supplement. Wish this research was going faster too…
I made this figure.
Having looked at many thousands of similar plots - this result is very striking. Will attempt to explain….
Daratumumab (anti-CD38) has partially reset autoantibody repertoires in this trial.
The cohort is small, but the reset effect occurs more in responders than non-responders.
What you typically see at paired timepoints looks like the “untreated” patients at bottom. Very tight and reproducible autoantibody repertoires across time. We and others have published on this. It is hard to get autoantibody repertoires to change (Bodansky et al 2024 shows BCMA CAR-T can do it, but not anti-CD20 - a B cell depletion that does not reset long lived plasma cells).
The plot is an intra-patient z-score scatter of raw HuProt protein microarray IgG autoantibody data before treatment, and then one year later. Each dot is a unique human protein. Most of the autoantibody events are private to individual patients. You can quantify these events to call “hits” with a simple binary cutoff (z>3).
Colored are unique antibody hits for patients in each sample pair. Blue occur ONLY at baseline, red pass threshold in both samples, yellow only post-treatment). You’ll note that all patients preserve a dominant autoantibody signature (red diagonal) demonstrating that the autoantibody reset is not perfect - the most dominant clones hold out in most patients.
You’ll note in the responder scatters “blue blobs” - these are the dozens of autoantibodies that go-away post therapy. You’ll note this blob looks a bit larger in the responders.
You can quantify the amount of this reset with a sort of Venn diagram ratio of target overlaps called a jaccard similarity. The untreated patients are about a 0.8/1 meaning nearly all the dots are red and all autoantibodies are shared at both timepoints by a simple binary categorization. I’ve seen that same ratio in thousands of other pre vs post timepoint autoantibody samples.
And thus, I find changes in that ratio quite striking! The treated non-responders have a median jaccard ratio about 0.5/1 and the responders about 0.3/1 which are the largest changes I’ve ever seen in HuProt data from the same individuals longitudinally. The amount of autoantibody hits that disappear also correlate with magnitude of patient improvement (SF 36PF scores, another slide from talk). The identities of the autoantibodies which disappear most is somewhat shared between the responders and also quite interesting- but will be up to the authors to reveal those results. Hard to be too certain about mechanistic autoantibodies as biomarkers in any study this small.
The trial is a bit small so it was hard to tell. There wasn’t a clear association to dose number which is good (responders got 4 or 7 doses). It could be “effectiveness of the depletion”, a pathogenic autoab remaining in non-responders that was cleared in responders.
Could also be that some cases are simply not antibody driven, and no amount of B cell depletion will fix.
@anna_reise87030@32Sfc46582 We have that data and will be part of the overall paper. There is a bit of an association between amount of antibody depletion and baseline NK cells
@Lorant661@RenzPolster Yep exactly anti-BCMA CAR-T might reset autoantibodies even better. Long term am hopeful you could “just identify the culprit autoantibody” and have a more specific therapy or tolerance vaccine that just fixes the issue vs resets all of antibody memory.
@SilenceUpNorth Yes - that is the hypothesis behind this trial. And we now have firmer - but not conclusive - evidence supporting that. The original trial report is here and the above should be published in the coming months:
https://t.co/SpRR863YTR
@mecfsskeptic Was quite excited they let me get so deep into the data! It’s theirs to publish, but our lab ran the samples and I’m more familiar with the datatype.
We build the world’s largest synthetic human proteome to screen for autoantibodies to 21K proteins all at once - every human we’ve ever tested has dozens to hundreds of autoantibodies - most private to themselves, stable for decades, unique between identical twins.
But it’s a long way from there to “proving they cause disease.” Most are to intracellular proteins and are perhaps harmless or help with cellular debris clearance. But things get very suspicious when cytokines, peptide hormones, etc are involved and people share them across a disease phenotype. Nearly every early pandemic sample long-COVID sample contains autoantibodies against the human protein MED20. So these things can become definable and diagnosable - but we need to make the libraries larger, the technology more scalable, etc.