LOVE Elephants, Giraffes, Dogs, Cats,and Goats! 😍 NOVID. STILL wearing a N95 😷 CovidisAIRBORNE. covidisVASCULAR. NOVOVAX FOR ANYONE WHO WANTS IT! ♥️ Poker
Pinning this to my profile for others!
I have now had 2 shots of novovax. So grateful to those who helped me figure out how to get it in this current, “you do you” era of the pandemic. 😷
😷 BREAKING🚨
Canada launches a new National Advisory Committee on Preventive Health Services.
It will be chaired by Dr. David Keegan, a leading advocate for masks in healthcare and on airplanes who filed human rights litigation on both fronts.
Während der Pandemie habe ich dem @rki_de früh mitgeteilt, das Patienten die nachts Luftfilter am Bett und damit keine 8h täglich mit kontinuierlicher Virus Reinhalation hatten, deutlich mildere #covid Verläufe hatten.
Nun bestätigt sich dieser Weg anhand von CT Bildern
Just stopped by the CVS Pharmacy and did my re-up. Folks in the USA, iirc you have a little less than half of the month to go for the deadline. This batch is done at the end of May
🚨📢The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) will be meeting on May 28th to discuss and make recommendations on the 2026-2027 COVID-19 vaccine formula; public comment is now open
🟣Meeting announcement:
https://t.co/wRUubchUka
🟣Public Comment link:
https://t.co/xWarvoj0DI
Public comment is open until May 27th, 11:59 PM EDT, but only comments received on or before May 21st will be provided to the committee.
🟣Some ideas for talking points, which I’ll personally be making:
💉All COVID-19 vaccines should be made available universally, with labeling not limiting use to high-risk populations, and free of cost.
💉Manufacturers should once again target a monovalent JN.1 lineage, preferentially XFG or NB.1.8.1. Any JN.1 lineage would be acceptable, due to similar antigenic grouping, but current evidence does not suggest that emerging BA.3.2 should be an antigen target at this time.
💉The strain selection process should be more frequent (at least twice per year, the same schedule as the WHO’s TAG-CO-VAC). Considering COVID-19’s lack of seasonality, it should also be scheduled earlier in the spring (in ~March, like influenza strain selection) and it should be a goal to release updated vaccines before children return to school in late summer.
💉Nuvaxovid’s indication should be expanded to include pediatric use, and Nuvaxovid’s shelf life should be extended from 6 to 9 months, in line with other COVID-19 vaccine products.
Of course, it’s best practice to always use your own words in your comments.
💉It has become integral for the VRBPAC to acknowledge the advantages of Nuvaxovid, which are undeniable at this point, along with the prospect of an updated priming series for those previously vaccinated with mRNA. Nuvaxovid has better coverage across variants, a stronger mucosal response, a higher quality of antibody composition, longer durability, and less reactogenicity, to name a few. Such an acknowledgement would serve to restore trust in public health and allow us to better take advantage of this new era of the COVID-19 pandemic, defined by lower transmission rates, lower death rates, and lower vaccine uptake, but with the continued significant threat of Long COVID.
Of course, it’s best practice to always use your own words in your comments.
Novavax reminder: You should probably be making plans to get your spring Nuvaxovid booster within the next week, if you’re planning on getting one.
Sanofi has confirmed this batch, expiring May 31st, will be the last availability until the release of the 2026/2027 formulation in the fall.
At the very least, confirm with a pharmacy that they’re planning on remaining stocked until the May 31st expiry. It’s common practice, unfortunately, for pharmacies to return inventory a few weeks before it actually expires, especially in the spring when there’s little uptake. This includes @cvspharmacy, which is responsible for the bulk of Nuvaxovid inventory right now.
🔬Study shows SARS-CoV-2 causes direct damage to heart cell mitochondria - even months after recovery - helping potentially explain Long COVID heart symptoms like chest pain, palpitations & fatigue.
Let’s break it down 🧵
Imagine how many more productive years of healthy living our kids could have if schools properly cleaned the air to mitigate airborne infections. Then, imagine what all of those extra healthy years would mean for economic productivity, @CAgovernor@GavinNewsom@GovPressOffice.
This is spot on! She does a terrific job of summarizing the science in a couple of minutes.
Worth a view, even if you’re cc. It’s a great way of connecting the dots.
A reminder about COVID-19 boosters, including Novavax / Nuvaxovid, since it comes up a lot this time of the year:
You are entitled to a 2nd seasonal dose as long as it has been more than 2 months since your previous dose.
However, there are only two official pathways where more than 1 annual dose is indicated:
1. Immunocompromised status
2. Being aged 65+
If you don’t end up having to mention either of those things, then you just happened to run into a “good” pro-vax pharmacy, but the immunocompromised rules (https://t.co/Ovt3mZM8IB) are what someone should be prepared to use.
As always, the immunocompromised rules are a self-attest system and pharmacies are not permitted to require documentation or deny you an additional dose. They may try, but refusal is reportable to your state’s pharmacy board, and that’s the type of situation they would like to hear about. They actually tend to be pretty quick about resolving these kinds of issues.
If insured, your insurance plan is also legally required to cover your dose. They don’t have a choice in the matter - that’s the entire reason for ACIP/CDC guidance. If a pharmacy (or any other medical provider) determines that you are eligible, which obviously needs to happen for you to get the shot in the first place, then that alone triggers the coverage.
@ValerieJay16 Curious, I tried for a booster last week and was denied. They had a brand new box that didn’t expire until May 2026. But I think the insurance rejected it…as it had only been 5 months. Has it been more than six months since you were boosted?
Scientists create universal nasal spray vaccine that protects against COVID, flu, and pneumonia
The new formulation, currently called GLA-3M-052-LS+OVA, is designed to replicate the T cell signals that stimulate innate immune cells in the lungs. https://t.co/83b6qtLy3F
https://t.co/PuFvE1YCKg
This new paper on the mRNA vaccines really helps to explain some of the benefits of Novavax. The main focus is on mRNA’s cardiovascular side effects (which is a separate issue), but what’s most interesting to me is that is helps explain why we get less protection against infection across variants with mRNA when compared to Novavax.
Those benefits are at least somewhat related to Novavax’s focus on CD4+ T cells and the S2 subunit of the SARS2 spike protein, which we did already know, but now we understand a key mechanism for WHY Novavax is so much better at it than the mRNA vaccines.
To start, a couple brief summaries/reminders:
1. How the SARS2 spike protein works: The spike is made up of 3 main parts - The NTD (N-terminal domain) and RBD (receptor binding domain) in the S1 subunit, and the S2 subunit. The vast majority of mutations happen on S1, while S2 is a lot more stable. Since S1 contains the RBD, which is where the virus attaches to our ACE2 receptors, it does tend to be more important to have the immune system mount a response to S1 epitopes for the purpose of preventing infection. However, S2 is still extremely important when trying to generate an immune response across multiple variants - since, like I mentioned before, S2 is a lot more stable.
2. How T cells work: CD8+ cytotoxic T cells are the cells that directly kill cells that are infected by a virus like SARS2. CD4+ Helper T cells are the cells that coordinate the entire immune response: they identify pathogens and signal to other immune cells (B cells, macrophages, and the aforementioned CD8+ T cells, etc.) to destroy pathogens.
Now, here’s what we learned and had confirmed in this new paper: Essentially, the mRNA vaccines can only induce a robust CD4+ response against the S1 subunit, and NOT against the S2 subunit.
Why?
The paper found that, after our body produces the spike protein post-mRNA vax, it gets broken back down into its two main parts - S1 and S2 - while still inside of our cells. After that breakdown occurs, only the S1 subunit was detected outside of the cells that were tested, while the S2 subunit remained inside of all of the cells tested.
Next, there are two main pathways that generate immunity: MHC Class I (intracellular) - which activates CD8+ cells, and MHC Class II (extracellular) - which activates CD4+ cells.
So, essentially, since S2 is not present extracellularly, the mRNA vaccines are not generating CD4+ cells (which are required for coordinating the entire immune response) primed against the S2 subunit (which is the key to maintaining a response across a wider range of variants).
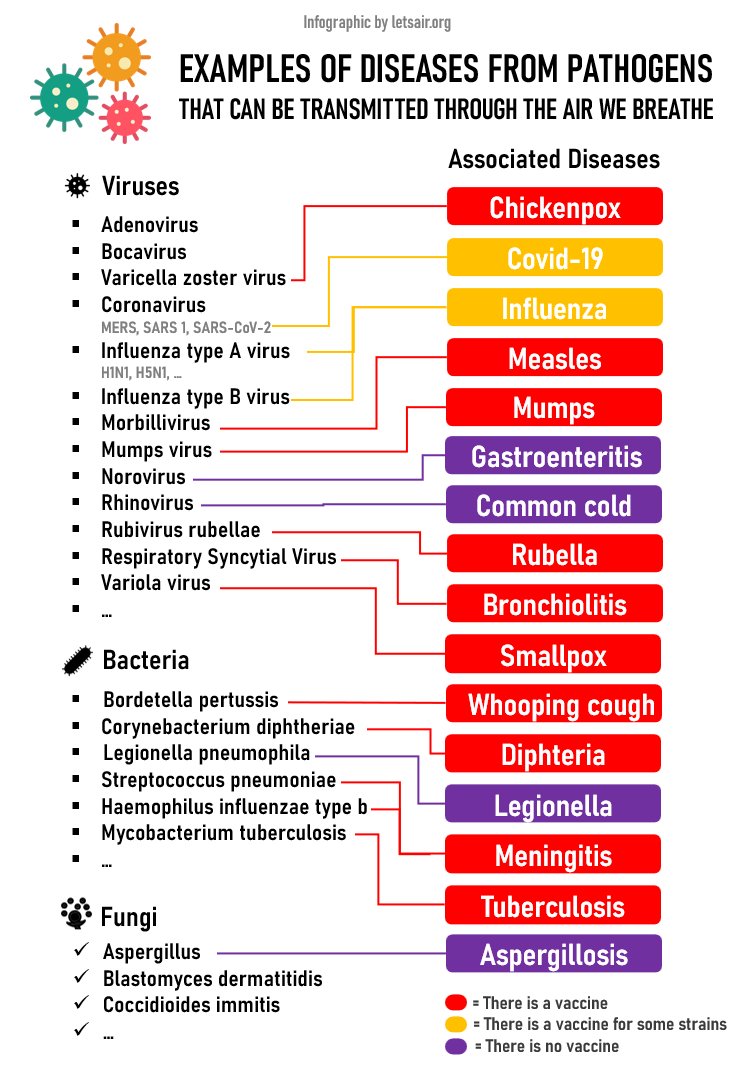
We've updated our infographic on diseases that can be transmitted through the air we breathe, adding Norovirus.
Most viruses can survive for one to several hours in a poorly ventilated room. See the excellent article in @nytimes on this topic: https://t.co/My5iX6kJ2b