Our paper describes a simple, low-cost "Screw-Lock" technique to securely fix the DBS burr-hole base ring when there is a size mismatch, improving lead stability in resource-limited surgical settings.
https://t.co/fNnmzknRjl
Stop wasting hours trying to learn AI.
One list.
Zero confusion.
No fluff.
I’ve already done the hard work for you 👇
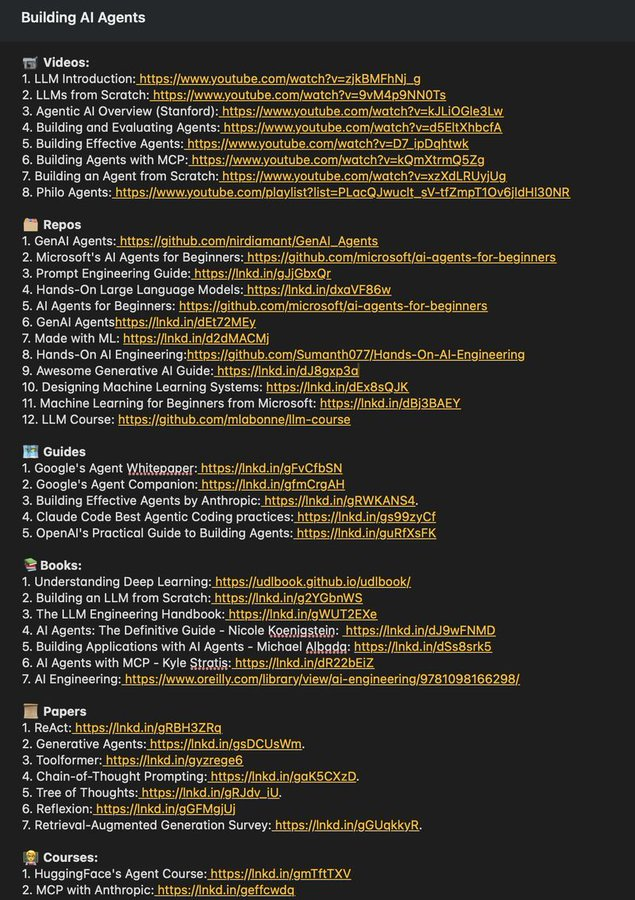
📄 Complete AI Learning Document
https://t.co/3h3k80FhZV
What’s inside:
📹 Videos
LLMs, Agentic AI, real-world breakdowns (Stanford + more)
🗂️ GitHub Repos
GenAI agents, prompt engineering, hands-on LLMs, beginner → advanced
🗺️ Guides & Whitepapers
Google, Anthropic, practical agent design
🧑🏫 Courses
Hugging Face, MCP, Vector DBs, end-to-end agent systems
📚 Books
From fundamentals to LLM engineering
📜 Research Papers
ReAct, Generative Agents, Toolformer, and more
📩 Newsletters
Stay updated without doomscrolling
Everything is curated, sequenced, and practical.
No random bookmarks. No hype.
♻️ Repost for your network
❤️ Like · 🔖 Save
➕ Follow for more on AI Agents & real-world GenAI
Ant-amyloid MABs are offerning hope for millions of sufferes of Alzheimer's disease in the world, In this editorial I raised few questions, which needed to be answered to acheive success in treating these patients.
https://t.co/OkeZmI0afY
Don’t get locked in when it comes to brainstem syndromes!!
Do you just say the lesion is in the pons or medulla & hope no one asks questions??
You can do better!!
Here is the anatomy that you need to know to understand brainstem syndromes and localize lesions on MRI!
You can see the tricks I use remember all the medullary syndromes here:
https://t.co/jIrPfSqCvC
And if you want an easy mnemonic for pontine syndromes, check out mine here:
https://t.co/LWrbmXtGFR
Hopefully, now you know this anatomy stem to stern!
Back by popular demand!!
Sagittal T1 is meant for anatomy!
Do you know it??
Most people know anatomy mainly in the axial plane. But the sagittal is actually perfect for anatomy
Sagittal shows the midline structures & makes gyral anatomy easy, bc gyri in the brain are structured like a layer cake.
And just how you see the layers in the cake best when it is cut on the side—you best see gyral anatomy when the brain is cut from the side.
For every sagittal T1, I have certain check points I check as I move through the anatomy.
This shows you my check points. How many do you know? How many do you have as you scroll?
Have MULTIPLE questions about MULTIPLE sclerosis?
Having trouble seeing neuromyelitis optica?
In a fog about MOG?
Here’s the cheat sheet you NEED to distinguish the demyelinating diseases!
Demyelinating diseases predominantly involve the optic nerves, brain, & spine.
Three main chronic demyelinating diseases:
🔸Multiple sclerosis (most common)
🔸Neuromyelitis optica (NMO)
🔸Myelin oligodendrocyte glycoprotein (MOG) antibody associated disease or MOGAD
Each has its own features in the optic nerve, brain, & spine. Here’s how to remember them!
▶️MS
🔸Optic nerve:
MS only has 2 letters, so MS involvement of the optic nerve tends to be short segment
🔸Brain:
Letter M makes the shape of the perivascular distribution of lesions along the ventricles (Dawson’s fingers)
Letter S makes the shape of the subcortical U fiber involvement
🔸Spine:
MS is only 2 letters, so lesions are usually less than 2 vertebral bodies in length
▶️NMO
🔸Optic nerve:
NMO is a longer abbreviation, three letters, so longer involvement
NMO can stand for Near My Occiput. Occiput is posterior, so more posterior nerve involvement
🔸Brain:
NMO can stand for Near My Ocean. What is your brain’s ocean? The ventricles. NMO lesions are all periventricular
🔸Spine:
NMO is 3 letters, so lesions usually more than 3 vertebral bodies in length
▶️MOGAD
🔸Optic Nerve:
Remember MO’ GAD-olinium. So things that cause more regions of enhancement. MOGAD lesions are commonly bilateral & long segment & enhancement can extend perineural
🔸Brain:
Remember LO’ GAD. MOGAD typically involves the lower areas of the brain
🔸Spine:
Remember MO’ PLAID. MOGAD can give a plaid-like H shape in the cord from predominantly gray matter involvement
Hopefully, this cheat sheet will help you remember how to distinguish the demyelinating diseases! It ain’t lyin’ about diseases of myelin!
Have some mild cognitive impairment trying to remember dementia patterns on imaging?
Is looking at dementia PET scans one of your PET peeves?
Have short-term memory loss when you read about dementia imaging?
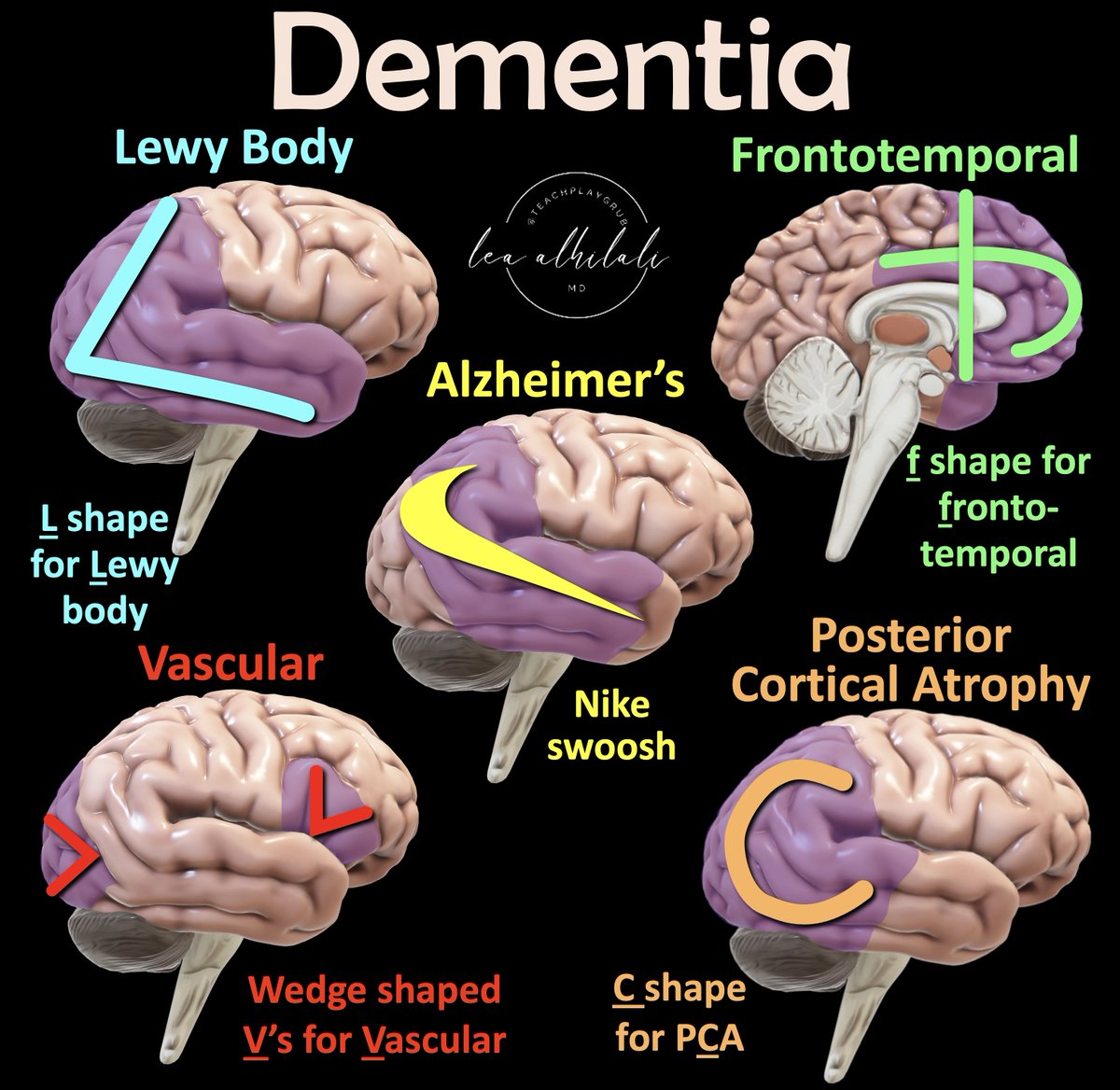
Here’s a way to remember dementia patterns so you will never forget!
Major dementia imaging patterns:
➡️Alzheimer’s disease (AD)
🔸AD has a Nike swoosh pattern—with decreased metabolism in the parietal & temporal regions
🔸Remember when you see the Nike swoosh patter, just call it!
➡️Dementia w/Lewy Bodies (DLB)
🔸Temporoparietal hypometabolism like AD but also involves occipital cortex, specific for DLB. DLB also extends farther to the ant. temporal cortex.
🔸Remember, regions of hypometabolism look more like an L. And Lewy starts w/an L
➡️Frontotemporal Dementia (FTD)
🔸Frontal & temporal hypometabolism as expected, but extends along the anterior cingulate gyrus
🔸Anterior cingulate involvement makes the hypometabolism looks like a lowercase letter f—and frontotemporal starts with f
➡️Posterior cerebral atrophy
🔸Can from AD or DLB & has hypometabolism in the occipital & post. temporal lobe, sparing the anterior temporal lobe
🔸Sparing the anterior temporal lobe makes the involvement look like a C instead of an L like DLB.
So remember pCa
➡️Vascular dementia
🔸Vascular dementia has a variable distribution, depending on the regions infarcted (V is both for Vascular & Variable)
🔸Wedged shaped regions of hypometabolism corresponding to cortical infarcts—looks like an inverted V
This list isn’t all inclusive & there can be variations or even mixed dementias
But hopefully this gives you a starting point you won’t soon forget!
Organising Your Neurology Diagnosis
The “NAPE” System
Neurology can initially seem daunting, but it’s the most logical system to analyse once you get the hang of it!
The NAPE System is an easy way to organise your thoughts
🧵
The neurologist I want to see when I get sick needs to be a generalist with a specialist eye, a humanist with a touch of the supernatural and a physician who finds as much to interest in a Bells Palsy as in a hereditary congenital facial paralysis. Scientism is not essential.
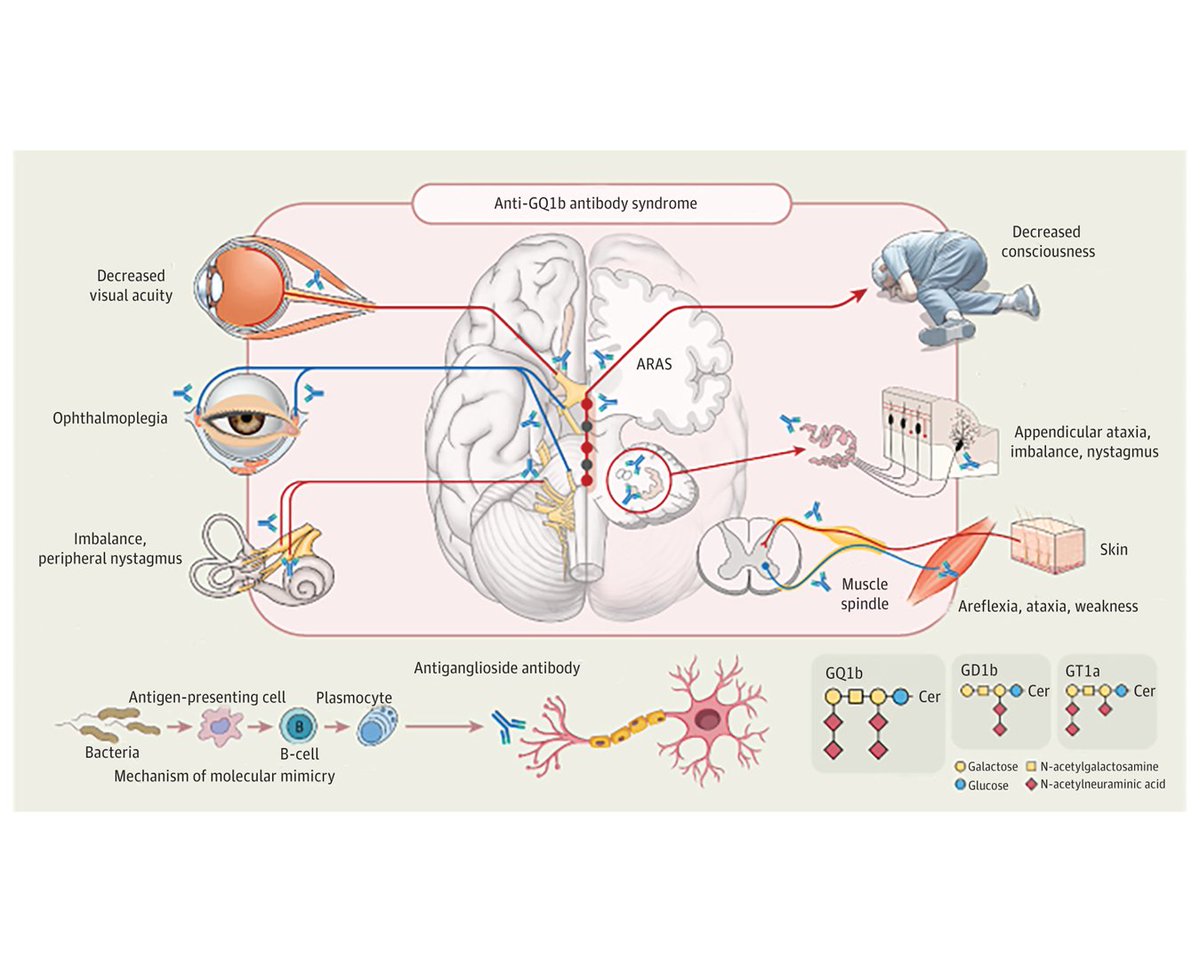
The clinical spectrum of anti-GQ1b antibody syndrome continues to expand to include acute vestibular syndrome, optic neuropathy, and acute sensory ataxic neuropathy in addition to classic syndromes. https://t.co/2z3WAXbTZt #MFS#GQ1b#Ophthalmoplegia
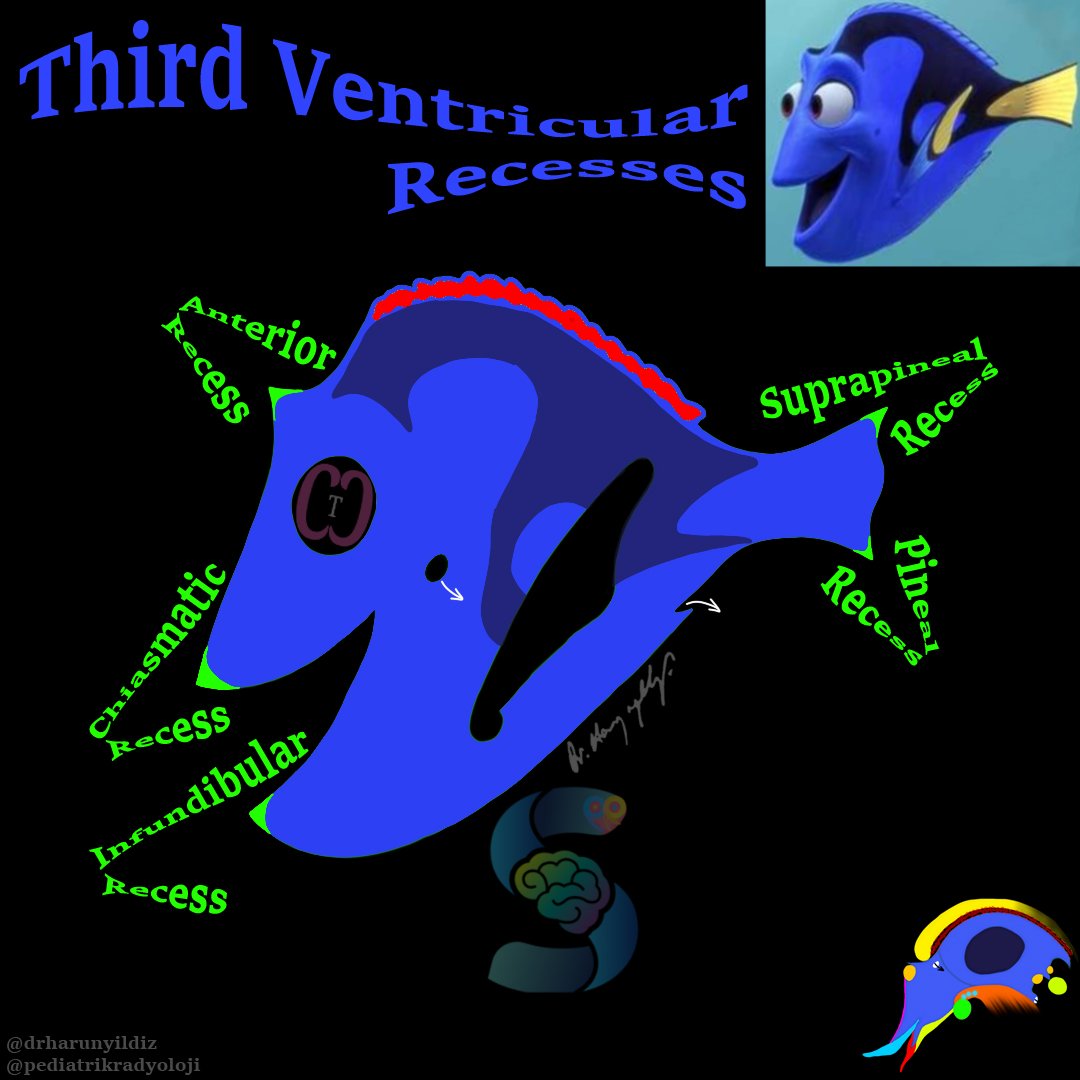
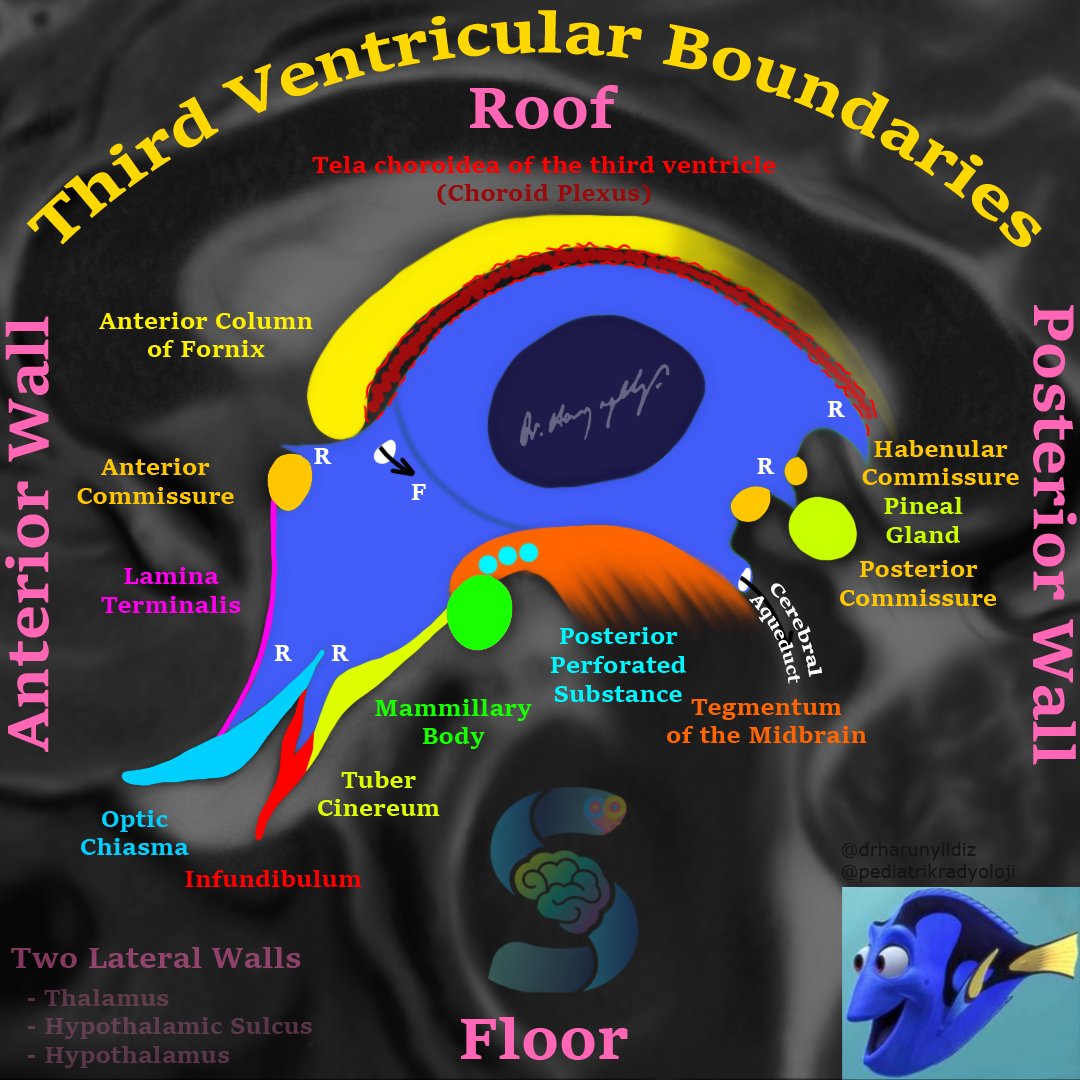
They say three’s a crowd!
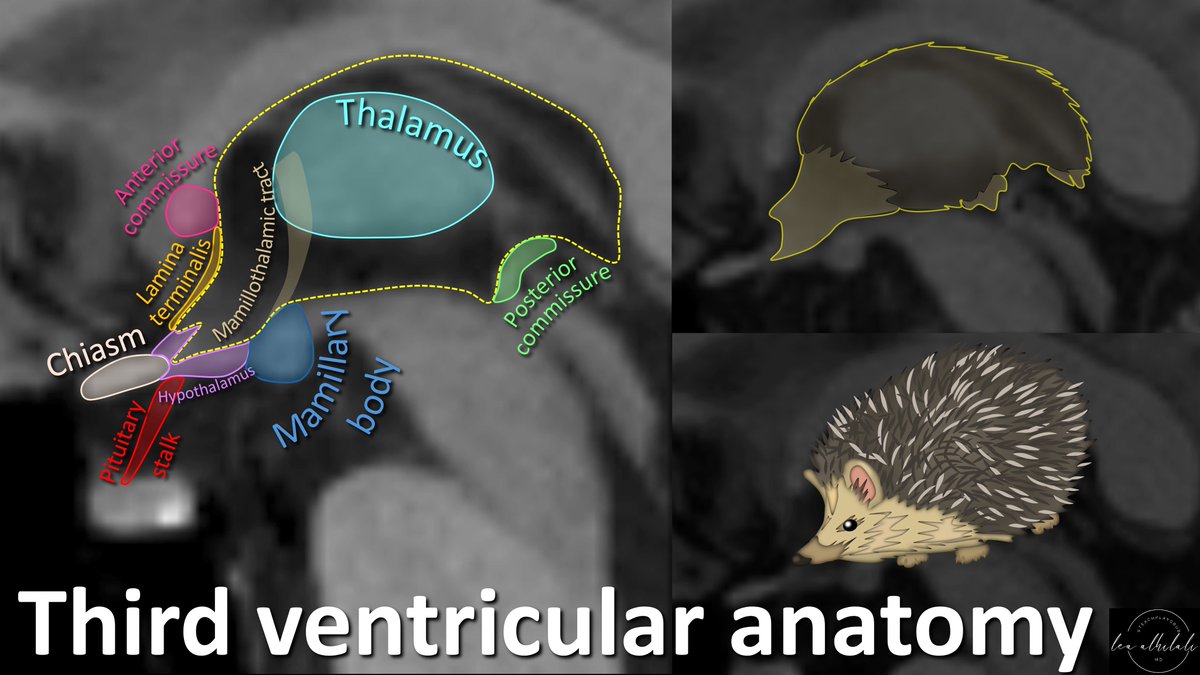
Anatomy at the 3rd ventricle is crowded by important structures!
How can YOU remember anatomy in this region?
3rd ventricle looks like a hedgehog.
And that hedgehog can keep you from hedging about anatomy here! Here's how it can help you remember:
Here are the important structure you need to know & how the hedgehog can help keep them straight:
➡️Anterior commissure is between the eyes (anterior = eyes)
➡️Posterior commissure is between the legs (posterior = legs)
➡️Hedgehog’s snout open onto the hypothalamus (snout = mouth & hypothalamus controls eating!)
➡️Mamillary bodies are near where the mammary glands would be in the hedgehog
➡️Lamina terminalis is along the nose—and where does your face TERMINATE? At the nose
Now you know the hedgehog of the third ventricle & how to remember anatomy in this region.
It’s as easy as one, two, three!
‘Every physician must be rich in knowledge, and not only of that which is written in books; his patients should be his book, they will never mislead him’
Paracelsus writing 400 years before Osler
@ChrisBoesMD@AndrewElder@gavinfranc @JohnLauner