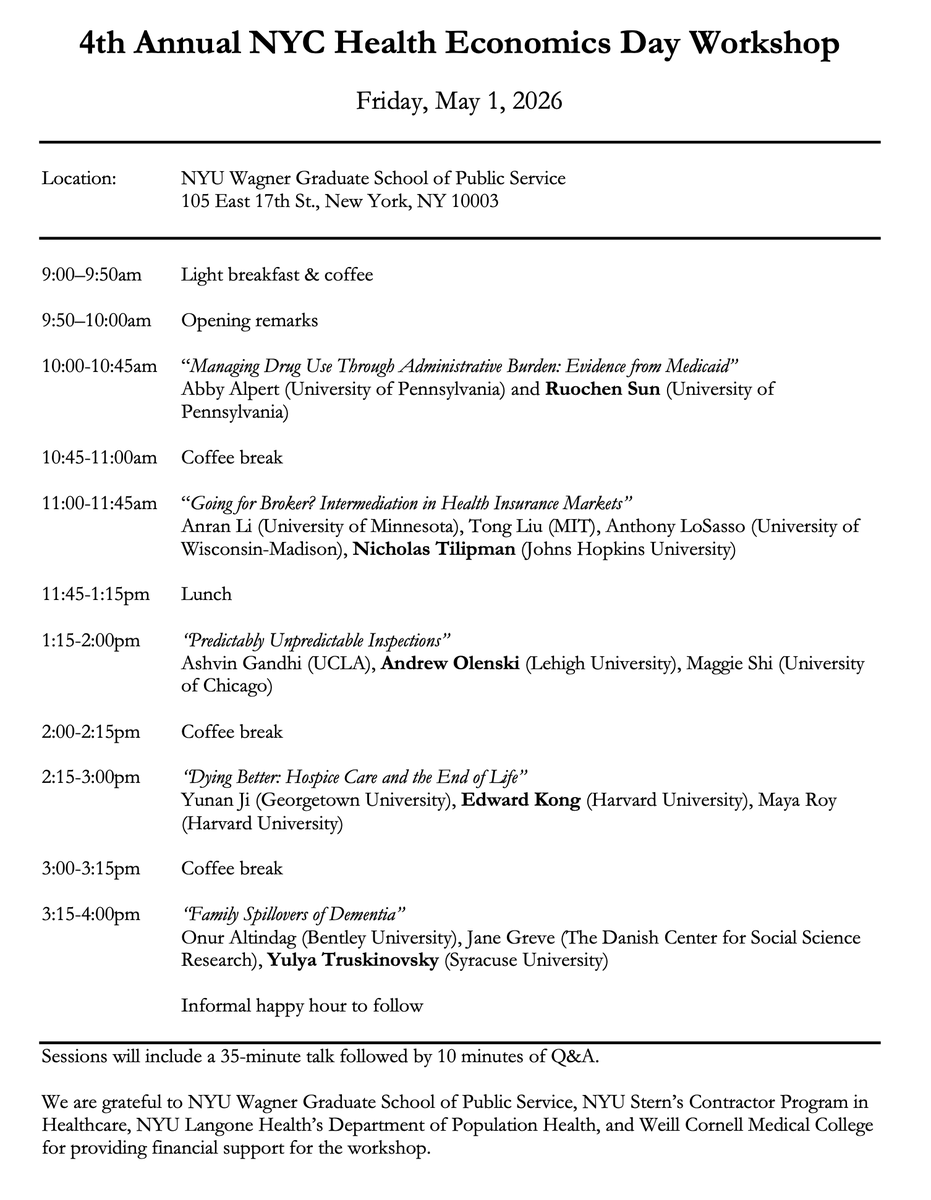
NYC Health Econ Day is coming to @NYUStern May 3! We'll have four great paper presentations with lots of time for folks to chat.
RSVP here: https://t.co/auwGRQ1fhp
More info: https://t.co/K74sGqdpdg
Organizers: @amy_m_bond@sunitamd@MJ_Dickstein@LaurawherryR + me
New study w/@leorahorwitzmd@Ateevm+ many others: RCT across NYU Langone practices to study the effects of real-time prescription benefits (RTPB) on out-of-pocket costs. https://t.co/vYIObsAnFK 1/7
Many thanks to wonderful mentors @Ateevm@leorahorwitzmd + a dynamic cross-functional team spanning operations, pharmacy, IT, and research + and @nyulangone for facilitating this RCT. It was my first RCT and a lot of fun! 7/7
Nonetheless, results suggest providing patient-specific out-of-pocket cost info at the point of order entry can influence rx. This stands in contrast to many consumer facing price tools which gained less traction. Engaging physicians on issues of cost and value is important! 5/7
We can’t really say whether the extra diagnostic codes reflect inappropriate upcoding or more accurate coding by the hospitals with higher private insurance mix. But our work does highlight a previous unexamined cross-payer externality. 3/3
Fun paper led by the dynamic @kacie_dragan. Does hospitals' private payor mix affect dx coding intensity in Medicaid? The idea was that hospitals with higher shares of private pts may have more incentive to invest in intensive coding infrastructure and practices. 1/3
On a personal note, this project is dear to me, as it’s a collaboration with some of my favorite people & mentors — together, all in one paper! (big thanks to Sherry, John, @sunitamd ) — and a very fond reminder of the fun I had at @NYUWagner !
We find yes, it does.Following Medicaid pts with admissions at >1 hospitals, the same pt was coded more severely when admitted at a hospital with a higher private mix. We did several analyses to try to get rid of potential sources of bias that could be driving our results. 2/3
Interesting paper by @sunitamd +team in @JAMAHealthForum. 340B gives drug discounts to hospitals that treat low-income patients. Instead, growth in 340B has in rich and white areas. Opposite of 340B's goal! https://t.co/cJMpo9K7zh
New @JAMA_current paper led by intrepid NYU resident @WaqasHaqueMD systematically reviewing 5,000+ hospital websites to measure compliance with the Federal Hospital Price Transparency Rule. This was such an impressive lift for an important question. https://t.co/jtoEkxfLba 1/3
Hospitals have unsurprisingly resisted, but oversight should not be hard, and the onus should be on hospitals to demonstrate compliance. Penalties were raised to $10/day/bed (up to $5.5K/day), but last I heard penalties haven’t been enforced. 3/3