Assistant Professor/Transplant Hepatologist; Fellow@MayoClinic, Rochester @MayoClinicGIHep, @CedarsSinai,@NIH/NIDDK.Tweets are mine, not medical advice
Pleased to share my promotion to Associate Clinical Professor of Medicine at the University of Arizona – Phoenix. Grateful to my mentors, colleagues, trainees, patients, and family for their support. Looking forward to advancing patient care, education, mentorship, and research.
Truly honored and humbled to receive the Faculty Mentor of the Year Award (2026) from University of Arizona College of Medicine/ Banner University Medical Center Phoenix. Teaching and mentorship have always been among the most rewarding parts of academic medicine.
Excited to share our recent publication in Transplant Direct highlights the impact of GLP-1 receptor agonists and SGLT2 inhibitors on post-liver transplant outcomes, including MACE, graft failure, renal outcomes &mortality
https://t.co/oQYMfw9iQ6
@UATransplantHep@UAzMedPhxChair
🔥 HOT TOPIC
📗 @HEP_Journal#HEPATOLOGY
Selected for its clinical impact, this meta-analysis delivers critical insights into which anti-diabetic therapies may also reduce liver-related events in patients with #MASLD.
For clinicians managing the complex overlap of #diabetes and liver disease, these findings could directly inform treatment decisions and improve patient outcomes.
Read the full study here: https://t.co/VXgqkJAhFQ
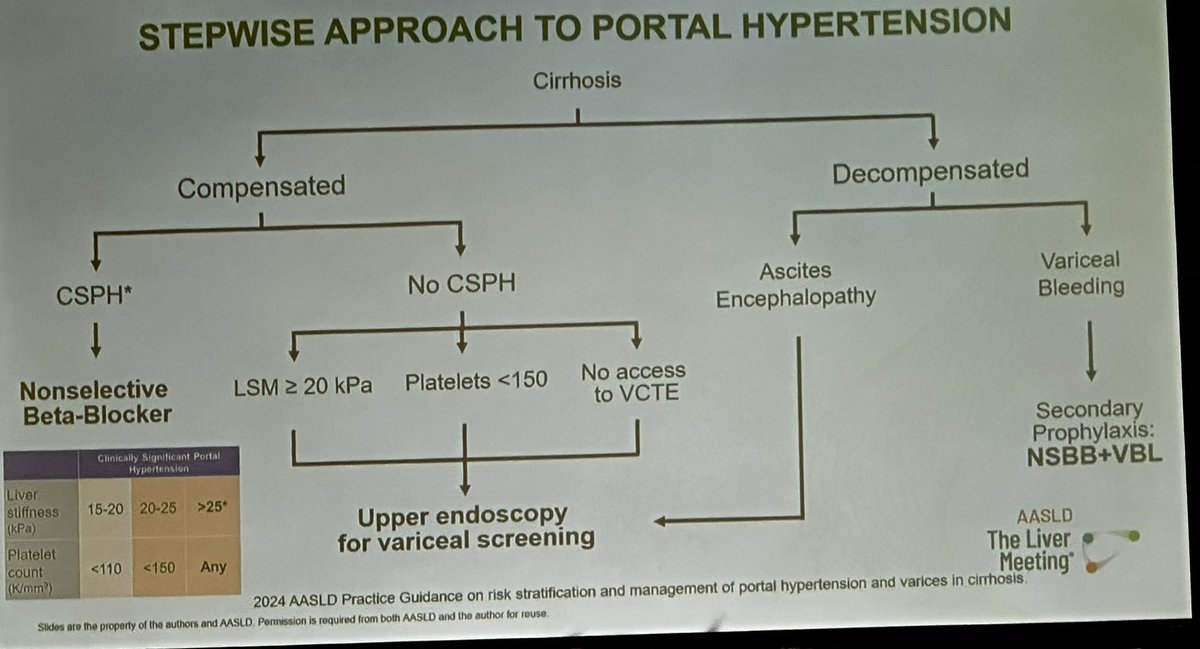
Real-world data in clinical practice
identify CSPH with VTCE & Plt
VTCE15-20+plt <110
VTCE 20-25+ plt < 150
VTCE >25 + any plt
NSBB for cACLD with CSPH
Telepression+Albumin - 1st line for HRS-AKI
Resp Failure Risks- ACLF3 & Hypoxia
#TLM25@AASLDtweets
Takeaway-Obesity Medicine Course -2 re: MALSD & MET-ALD
-importance to recognize effect of alcohol on post bariatric Sx- emerging MET-ALD
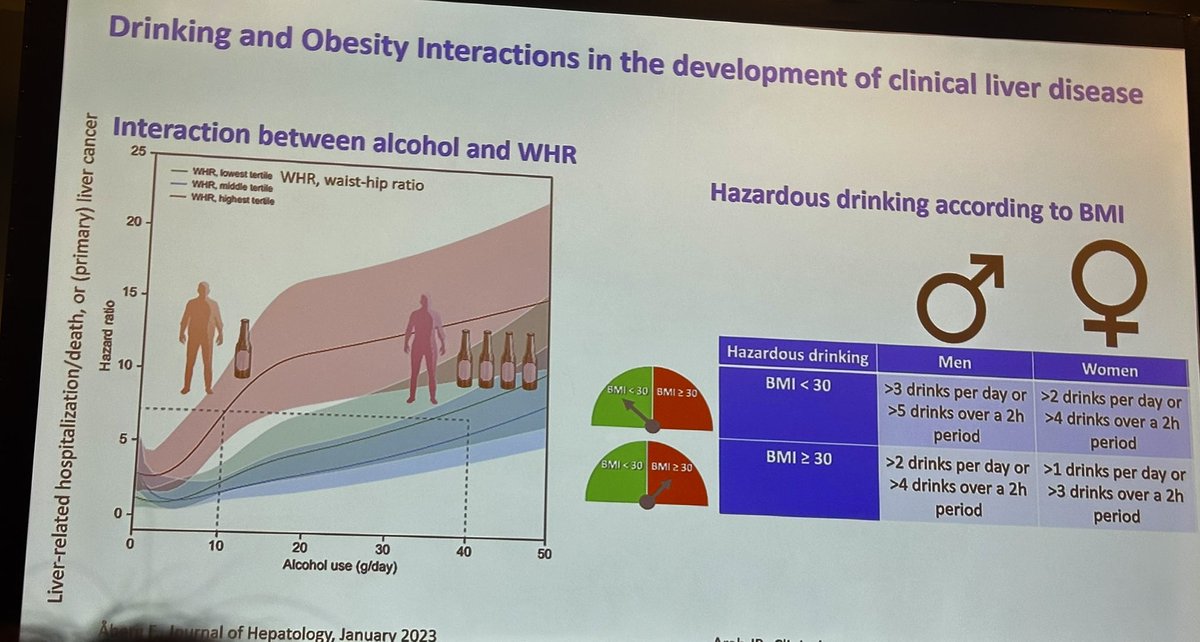
- Drinking & Obesity in development of ALD
- High Protein diet is important to prevent obesity sarcopenia
@AASLDtweets#TLM25
Takeaway - Obesity Medicine Course 1 re: MASLD/ METALD
- address -addiction behavior to food cravings/Binge eating Do and alcohol
- Obesity - not just BMI, clinical manifestation is important in Mx #TLM25@AASLDtweets
The 2025 AASLD/IDSA Practice Guideline on the treatment of chronic hepatitis B was released on their website on November 4, 2025.
Here’s what has changed compared to the previous 2018 guidelines, according to ChatGPT.
🔴Pregnancy — antiviral prophylaxis to prevent mother-to-child transmission (MTCT)
• 2018: Suggest antiviral therapy in the third trimester for women with HBV DNA >200,000 IU/mL; TDF preferred in pregnancy; antiviral prophylaxis could be stopped at delivery or up to 4 weeks postpartum.
• 2025: Strong recommendation to start TDF (preferred) or TAF for persons with HBV DNA >200,000 IU/mL, optimally at gestational week 28 (third trimester). Adds that TAF has accumulating safety data and that earlier start (week 16) may be considered when infant HBIG is not available; recommends that prophylaxis can be stopped at delivery if there is no ongoing maternal indication, and gives detailed monitoring after discontinuation.
🔴Drugs preferred in pregnancy
• 2018: TDF preferred (TAF was newly approved but data limited for pregnancy); lamivudine/telbivudine shown to reduce MTCT historically but TDF preferred.
• 2025: TDF (preferred) or TAF (safety data reviewed) — TAF specifically acknowledged as an option with data cited. Notes insufficient safety data to recommend entecavir in pregnancy.
🔴Timing of prophylaxis (earlier initiation / special circumstances)
• 2018: Recommended third-trimester (generally) for high viral load; postpartum monitoring advised.
• 2025: Keeps week-28 initiation as optimal but adds: consider starting at week 16 to control viremia when infant HBIG isn’t available (new RCT evidence cited); also suggests earlier initiation if invasive procedures (e.g., amniocentesis) are anticipated.
🔴High-risk transmission (HBsAg+ persons in settings with risk of infecting others)
• 2018: Emphasized counseling, vaccination of contacts, and reducing exposure; antiviral therapy for prevention considered in pregnancy/high-risk situations.
• 2025: For viremic persons not meeting disease-specific treatment criteria but in high-risk transmission scenarios, the guideline suggests shared decision-making about antiviral therapy (conditional, very low certainty). Implementation considerations expanded (vaccination status of contacts, immunocompromised contacts, etc.).
🔴Immune-tolerant phase (HBeAg+, very high HBV DNA, normal ALT)
• 2018: Generally did not recommend treatment for true immune-tolerant adults; treatment was recommended for immune-active disease; caution about treating children/adolescents — monitor for transition. (Third-trimester pregnancy guidance separate.)
• 2025: Refines the approach: suggests antiviral therapy for immune-tolerant persons >40 years or those with significant inflammation (≥G2) or fibrosis (≥F2); for persons <40 years without fibrosis/inflammation the guideline recommends shared decision-making and periodic monitoring. (So the 2025 guidance provides clearer age/fibrosis/inflammation thresholds.)
🔴Indeterminate phase (HBeAg-negative, non-cirrhotic with intermediate labs)
• 2018: Recommended individualized decisions; monitor and treat when meeting immune-active criteria.
• 2025: Explicitly recommends shared decision-making for these HBeAg-negative, indeterminate patients and emphasizes reassessment at each visit if treatment is deferred (conditional recommendation, very low certainty).
Excited to be attending #TLM25 this year! It’s where hepatology professionals from around the world come together to share discoveries and impact the future of liver health. Register on-site (until Nov. 10th) or here 👉
https://t.co/h4WMoAG1ut @AASLDtweets@AASLDFoundation