#PathTip#GUpath#LPpath:
when screening prostate biopsies at low power &👁️ small glands traversing from one side of the core to the other ("glands crossing the street"):
definitely🛑stop &📷 go down on high power!
Low-grade B-cell lymphomas may present with prominent reactive inflammatory infiltrates or coexist with autoimmune disorders
⚠️ Increased IgG4:IgG ratio? Stop and think before diagnosing IgG4-related disease. Always exclude an associated lymphoproliferative disorder
What is the cause of abundant IgG4 in lymphomas?Possible explanations...
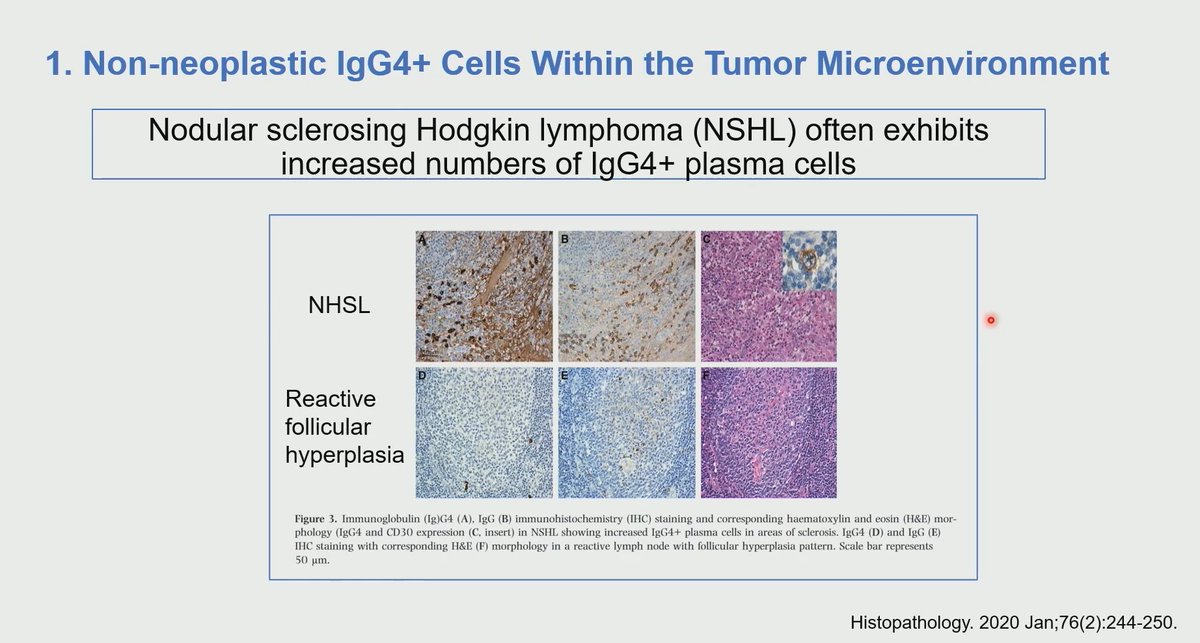
1. Non-neoplastic IgG4 cells within the tumor microenviroment
2. Monoclonal IgG4 production by lymphoma
3. Lymphoma can coexist with IgG4-related disease and other autoimmune disease
Dr. Herrera Hernandez #USCAP2026 #pathology #PathX #PathTwitter
#HilaryBuckleyAward Unilateral ovarian metastasis from lung adenocarcinoma with fibroma-like stromal proliferation: A diagnostic mimic of primary ovarian tumour. #BAGP2026
Mastocytosis (seen here) is often sought by naive colleagues and seldom seen. Mod Pathol offers a great review:
Panarelli NC, Hornick JL, Yantiss RK. What Is the Value of Counting Mast Cells in Gastrointestinal Mucosal Biopsies? Mod Pathol. 2023 Feb;36(2):100005. PMID: 36853780.
Our SW UK trainees asked me to teach for an hour and a half about gastric biopsies, so I short changed them and spoke for 1hr 29mins. Thanks to Shaun Walsh and @LizMontgomeryMD for some of the slides
https://t.co/JoMcDdkns7
#HemeOncHeroes series. Story #6
In 1955, childhood leukemia was almost uniformly fatal.
The pediatric leukemia ward at the National Cancer Institute @theNCI carried the smell of antiseptic, transfusions blood, and infection.
🧵 1/14
pic: Emil J Freireich, MD. The hematologist who refused to accept how children with leukemia died.
La displasia epitelial oral sigue siendo un reto diagnóstico por la subjetividad de varios criterios histomorfológicos.
Comparto un esquema visual basado en OMS 5ª edición y Hankinson et al. para integrar sus principales hallazgos arquitectónicos y citológicos.
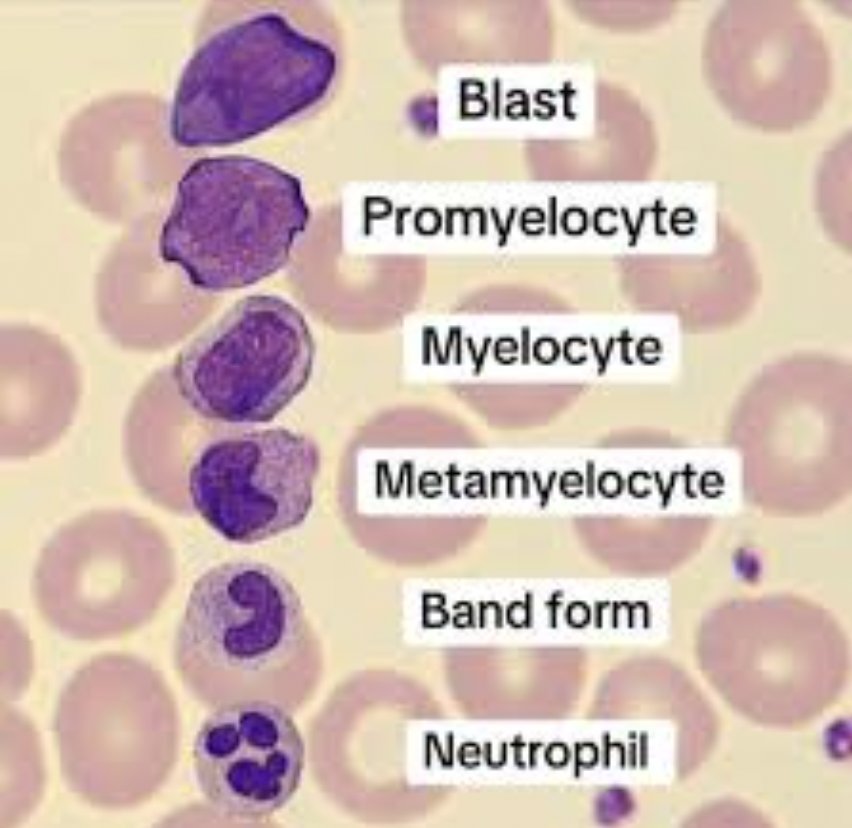
36 yr old, presents with anemia on D+80 post 10/10 MUD for AML.
Other lineages normal. Complete donor chimerism at D+60
Hgb: 78 g/L
LDH: 218
BM aspirate shows 👇🏽
📸 @ASH_hematology image bank
We are excited to launch the new @pathologyCast website:
🌐 https://t.co/YuEvyboogA
A modern, Netflix-style platform for pathology education featuring:
🔹 300+ lectures
🔹 Global expert speakers
🔹 100% free
Built to make pathology learning easier to explore, and enjoy
.
Second day of the first weekend of CAP #JobPrepBootcamp!
***Ovarian tumor frozen sections***
Clear cell carcinoma with adenofibromatous pattern can be signed out on frozen as “atypical epithelial proliferation in an adenofibromatous background”, defer to permanents (especially if atypia is focal)
Helpful tips for real-world practice!
#PathTwitter #JobPrepBootcamp #pathology #pathresidents #pathfellow #NIPPathX
Sarcomas that metastasize to lymph nodes should “SCARE” you!
These are:
S Synovial sarcoma
C Clear cell sarcoma
A Angiosarcoma
R Rhabdomyosarcoma
E Epithelioid sarcoma
#BST#sarcoma#Dermpath#boards#pathtwitter#pathx#mnemonic
Invasive fungal rhinosinusitis 🧫
Focus: what the pathologist must not miss in the report
Brief but potentially lethal: invasive fungal rhinosinusitis (IFR) is the form in which the fungus leaves the mucosa and invades submucosa, vessels, and bone, especially in neutropenic patients, decompensated diabetics, and transplant recipients.
Definition 🧬
IFR is histologically defined by invasion of the mucosa/submucosa by hyphae, with or without angioinvasion, clearly distinguishing it from non‑invasive forms (fungal ball, allergic fungal rhinosinusitis).
Histopathology 🔬
Architecture: nasal/sinonasal mucosa with necrosis and acute or mixed inflammation, often with “empty” areas of necrotic tissue permeated by hyphae.
Hyphae
📌Mucorales: broad, pauciseptate hyphae with irregular, often right‑angle branching (frequently collapsed on H&E).
📌Aspergillus: thin, septate hyphae with dichotomous, acute‑angle branching.
Vessels: thrombosis, necrosis of the vessel wall, and intraluminal invasion are the hallmark of the acute form; this explains the “black turbinate sign” on MRI.
Immunohistochemistry and special stains
H&E + Grocott–Gomori: highlights hyphae and their extent in vessel walls/bone.
PAS: useful, but less sensitive in extensive necrotic fragments.
IHC is occasional (for example, MUC5B, maspin in studies), not routine; the gold standard remains H&E + silver stain.
Diagnostic pitfalls ⚠️
Superficial biopsy with only crust/necrosis and no submucosa: high risk of calling “fungal colonization,” underestimating true IFR.
Necrosis without demonstrable hyphae: cut deeper levels, request Grocott, and if still doubtful, suggest a new biopsy in correlation with clinical/imaging data.
Confusing chronic invasive forms (Aspergillus, mucormycosis in diabetics) with tumor: solid masses with bone invasion can mimic malignant neoplasms.
What must be in the pathologist’s report 🧾
Explicitly state whether there is invasion of mucosa/submucosa and vessels by hyphae.
Suggest the likely genus (Mucorales‑type vs Aspergillus‑type pattern), with a recommendation to correlate with culture/PCR.
Indicate that the finding is compatible with invasive fungal rhinosinusitis and justify the urgency of clinico‑radiologic correlation and combined surgical + antifungal management.
Take-Home Messages NotasDePatologia
📌IFR is, above all, a histologic diagnosis of invasion, not merely of the presence of fungus.
📌Hyphae in vessel walls/lumina explain necrosis and worse prognosis; describe this clearly in the report.
📌Superficial, crust‑only biopsies are the main trap; ask for new material when necessary.
Selected References
Roland LT et al. Int Forum Allergy Rhinol, 2023 – AIFS consensus on pathology, imaging, and management.
Pagella F et al. J Cranio-Maxillofac Surg, 2016 – Acute vs chronic IFRS, clinicopathologic correlation.
Kurokawa M et al. RadioGraphics, 2022 – IFRS routes of orbital/cavernous invasion and imaging–pathology correlation.
⚠️Disclaimer⚠️
This text is an educational summary for healthcare professionals and students; it does not replace full pathology reports, local guidelines, or individualized clinical decision‑making.
#Pathology #HeadNeckPathology #InfectiousDisease #FungalSinusitis #InvasiveFungalRhinosinusitis
#SurgicalPathology #Histopathology #ENT #MedEd #MedicalEducation #NotasDePatologia
The references in this article are very thoughtfully curated. I’d highly encourage you to look them up and read them for a deeper understanding of the topics discussed in this paper.