MD PhD Consultant cardiologist. Evidence based medicine and ice hockey enthusiast. Married to Renathe. Father of three. Kapp. Toten. Bergen. Eidfjord. Norway.
@oyvlie Not many, I suppose.
Well, so now we have one type of HFpEF meds reducing HHFs but not symptoms, and one type reducing symptoms but doesn't do anything about HHFs. Better take both, then.
@drjohnm
@oyvlie@drjohnm@kjetil_loland I get your point. But we really have to look at the grand total: What is the net clinical benefit for the hfpef patient without crf and/or dm taking a sglt2i? Which, by the way, also goes for CV death - how many people care about what they die from? And at what cost?
@oyvlie@drjohnm@kjetil_loland Well, the question remains whether the endpoint is of any real importance for the patient, who likely does not care in which department he or she is admitted. Same for CVD death - who cares if the patient dies from CVD or any other cause - after all you are dead?
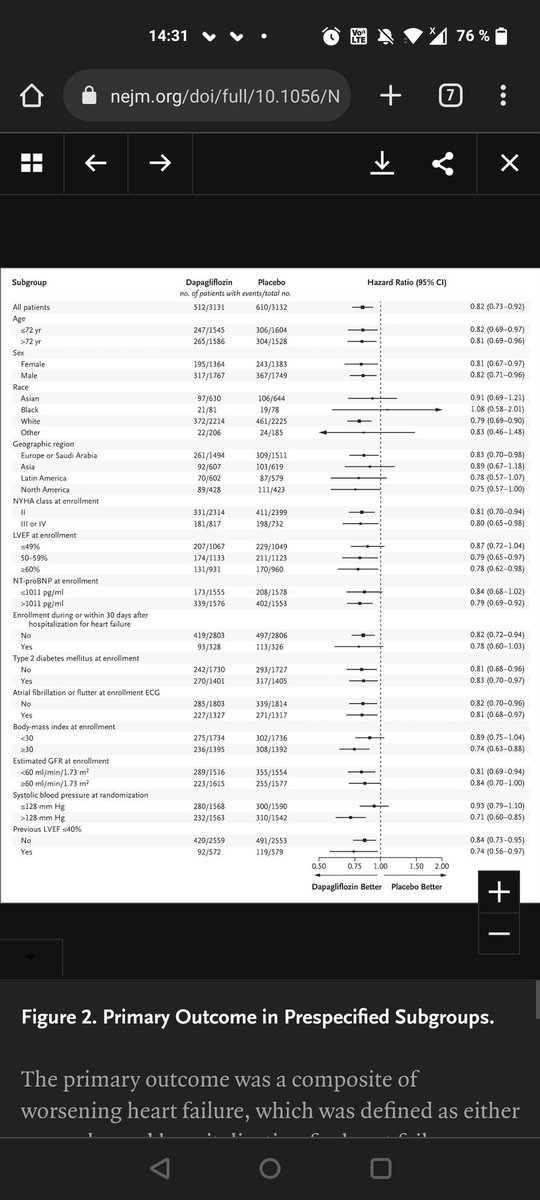
Regarding the DELIVER trial and endpoint statistics: Why was not win ratio used for the primary composite endpoint, when used for KCCQ? And why use rate ratios for CV death & HHF, potentially hiding any effect by time to event? @drjohnm@NEJM
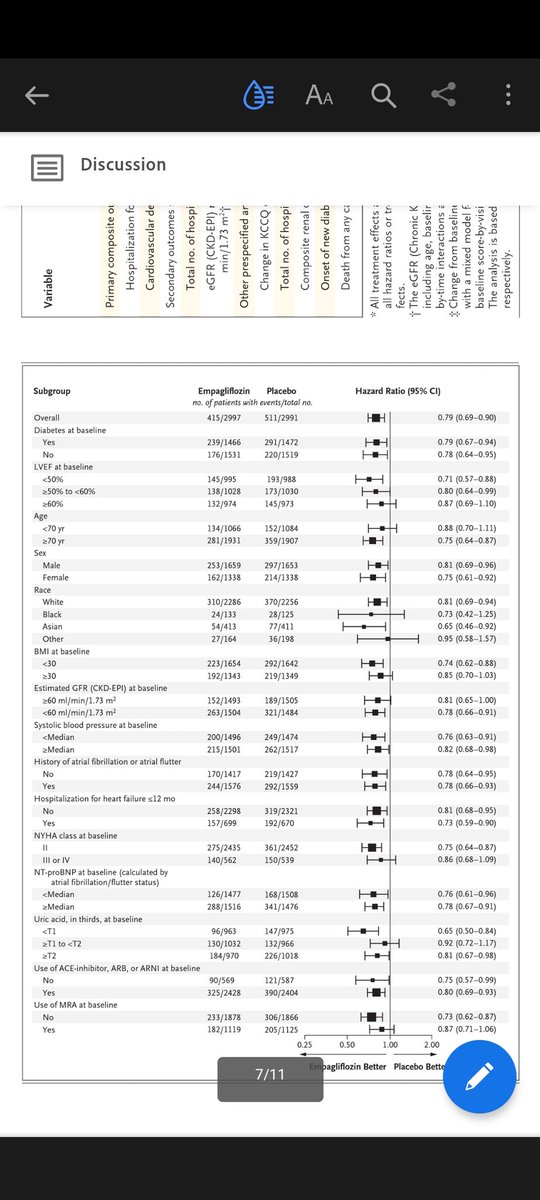
More SGLT2i and HFpEF: Why did not ppl w DM fare better off? They should have, just because they had DM (acc to Empareg outcome and other SGLT2i trials in pts w DM)? @drjohnm@NEJM@Diabeteslegen
@drjohnm Oh, and another thing. Total death events were around 400 in EMPA Preserved and about 500 in DELIVER. These number surely must be sufficient regarding statistical power?
@drjohnm 2. competing risk, especially for death. It ponders me how a drug (which is truly a game changer in DM and HFrEF) doesn't seem to alter BNP much, nor is the KCC moved much either. Yet, HHF is reduced.
@drjohnm 1. In my op, HFpEF is similar to NSTEMI (where invasive therapy against so-called 'culprit lesions' foesn't really do much). The condition occurs more often among elderly, multimorbide patients (DM, HT, AF, COPD etc), and is a marker of bad prognosis with tremendous amounts of
Prof Van Spall (Canada) questions the assumption of proportional hazards in Cox analyses in the DANCANVAS trial. Times are achanging. For the better. #ESCCongress