Real case: very low-risk prostate cancer (PSA 3.4 ng, Gleason 3+3, 2-12, ISUP 1) appropriate for active surveillance. A family seeks a second opinion; a surgical oncologist orders a PSMA PET-CT? and refers to medical oncology. The scan, performed at a low-experience center, is read as metastatic (bone and nodal), leading to unnecessary chemotherapy + ADT + ARPI.
When the patient returned to me, the findings did not match the clinical picture, so I recommended a second nuclear medicine review. Conclusion: rib and cervical “lesions” were inflammatory/benign uptake, not metastases. Likely technical issue: residual sodium fluoride in an aged PSMA radiotracer causing nonspecific bone uptake. No CT structural correlate.
Key takeaway: Integrate clinical context, pathology, and technical quality.
#prostatecancer
Great case!
Something similar is described in this RadioGraphics:
https://t.co/6NAkHkyIRq
Wasn’t aware it’s more common in younger patients
Thanks for sharing! @jonherochung
What is the real α/β in Prostate Cancer?
In this meta-analysis in the 🟢 Journal on regard BRFS :
α/β = 1.5 → no correlation
α/β = 3 → everything changes (R² 68%)
Practical translation : we don't know the real α/β value
#radonc
Celebrity alert: Troy is an MD Anderson #radonc resident and the lead author of the updated Revised STARS study reported at #ASTRO25 with a median f/u time of 10y showing no measurable benefit of surgery for stage IA NSCLC.
cc @JoeChangMD
The final sentence in this abstract could just as accurately conclude with "Given the limitations of this study, further investigation is warranted to identify the utility of surgery for octogenarian patients when SBRT is inherently safer in this population". Why? Because far too many patients over 80 have died within a few weeks of surgery for stage I NSCLC, including some of mine, driven by a "belief" that surgery is the better treatment.
Including the many whose fatal complications aren't even reported in this mansucript.
https://t.co/kqRcrE0JEC
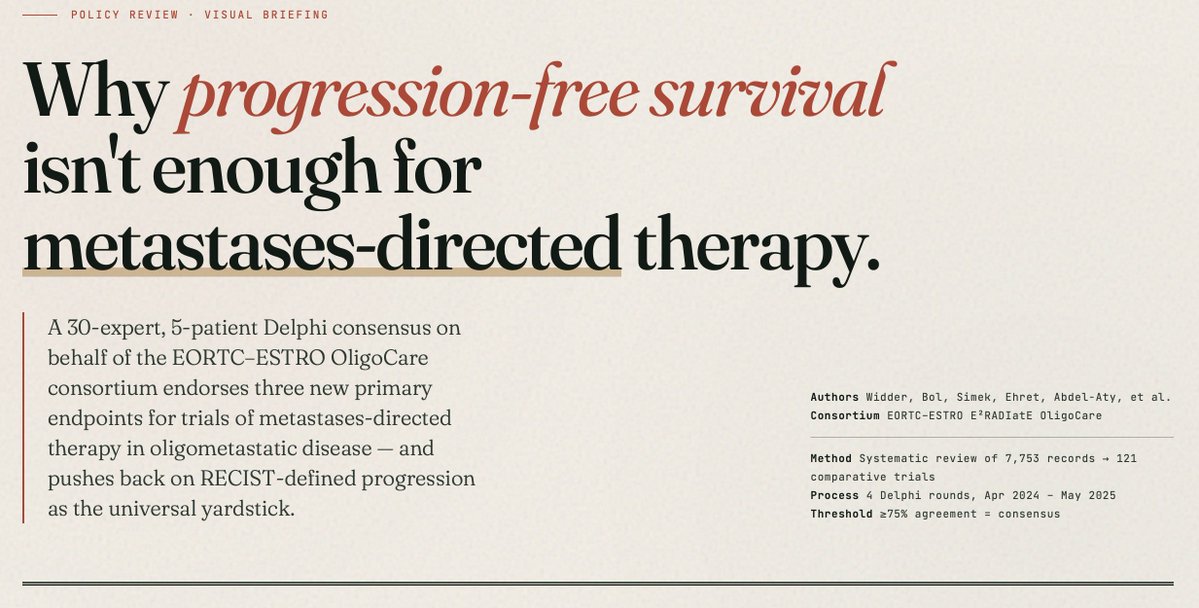
1/7 🧵 New in @LancetOncology: we built a Delphi consensus on primary endpoints for MDT trials in oligometastatic cancer — because the endpoints we've been using were designed for drugs, not for ablation.
On behalf of the EORTC–ESTRO OligoCare consortium.