#ASCO26#AML#leusm
Does venetoclax duration matter in frontline HMA+Ven for AML?
Poster: In a @MayoCancerCare analysis of 540 newly diagnosed AML patients, outcomes were driven primarily by disease biology, not venetoclax duration. Led by Dr. Naseema Gangat 👏👏👏
🔹 Similar OS across 7-, 14-, 21-, and 28-day schedules
🔹 Comparable outcomes within ELN 2024 and Mayo genetic risk groups
🔹 Higher early mortality with shorter durations likely reflected selection of frailer patients
🔹 In ELN high-risk AML, 14-day venetoclax was associated with inferior survival compared with 21- and 28-day schedules
Take-home: Venetoclax duration should be individualized based on genetics, response, cytopenias, and patient fitness rather than a one-size-fits-all approach.
🚨 NEW PUBLICATION 🚨
https://t.co/y6SzOVI3p6
CAR-T Exhaustion = A Major Barrier to Durable Remission 🧬⚡
CAR-T cells are powerful, but even engineered T cells can become exhausted.
Relapse after CAR-T is not always just antigen escape. Sometimes the engine burns out.
Key biology of CAR-T exhaustion:
• Tonic signaling before tumor contact
• CD28 vs 4-1BB = speed vs persistence
• PD-1/TIM-3/LAG-3/TIGIT = clues, not the whole story
• TOX/NR4A/BATF help lock in dysfunction
• The TME can starve, suppress, and reprogram CAR-T cells
What it looks like:
• poor expansion
• loss of persistence
• impaired tumor killing
• relapse after initial response
🧪 Next-gen strategies aim to keep CAR-T cells functional longer with smarter CARs, gene editing, armored CARs, rational combinations and more.
CAR-T failure is not one problem.
It’s a systems biology problem.
Check out our new @FrontImmunol review for more:
https://t.co/y6SzOVI3p6
#CARTcells #Lymphoma #Immunotherapy #CellTherapy #HemeTwitter
Scarisbrick et al - PROCLIPI
- prospec CTCL registry, 549 adv stage
- 5y OS 50%, IIIA better
- Prog factors: Age >60, N3, LDH incr, large cell Tx in skin
- Assoc with OS, PFS
- HRQoL also assoc
v useful as current staging system difficult & does not prognosticate
#ASH2025#lymsm
Original Article: Teclistamab plus Daratumumab in Relapsed or Refractory Multiple Myeloma (MajesTEC-3 phase 3 trial) https://t.co/DixpsZY8uT
#ASH25 | @ASH_hematology
This prospective international analysis demonstrated a real-world t(11;14) detection rate of 22.1% in patients with MM. Read in Blood Advances: https://t.co/Z0G0pR2QXH #MultipleMyeloma#BloodAdvances
All the major risk stratification models for myeloma, MGUS, SMM, WM, amyloid in one place!
Open Access! @LeukemiaJnl@ZanwarSaurabh https://t.co/oZnpRZySFt
Just out in the New England Journal of Medicine!
Our comprehensive Review on MGUS: Monoclonal Gammopathy of Undetermined Significance @NEJM https://t.co/7dza0YrFh5
5% of people over age 50 have MGUS. Every physician needs to know and understand MGUS. Lots of Tables and Figures. Bookmark!
How to test and manage patients. Who needs bone marrow exams and scans. It’s all in here!
MGUS is important not just because it’s a precursor to multiple myeloma. It causes a lot of other problems. Learn all about MGUS, and the various terms you hear MGCS, MGRS etc. in this Review
@myelomaMD and I have tried to keep every sentence in this Review simple and easy to follow. #MGUSVR
The tumultuous development of venetoclax in t(11;14) multiple myeloma
Just out in @JCO_ASCO
Preview below 👇🏻
https://t.co/XlBf4qxaFq
@MyMKaiser@OncoAlert
1/ New @BloodAdvances treasure trove of 🇩🇪 🇺🇸 data about bridging before CAR-T in #MMsm.
Bigger is not better when it comes to bridging using chemotherapy...
Worse post-CAR-T efficacy (unsurprising: tumor biology as confounder) but also clearly worse cytopenias & infections!
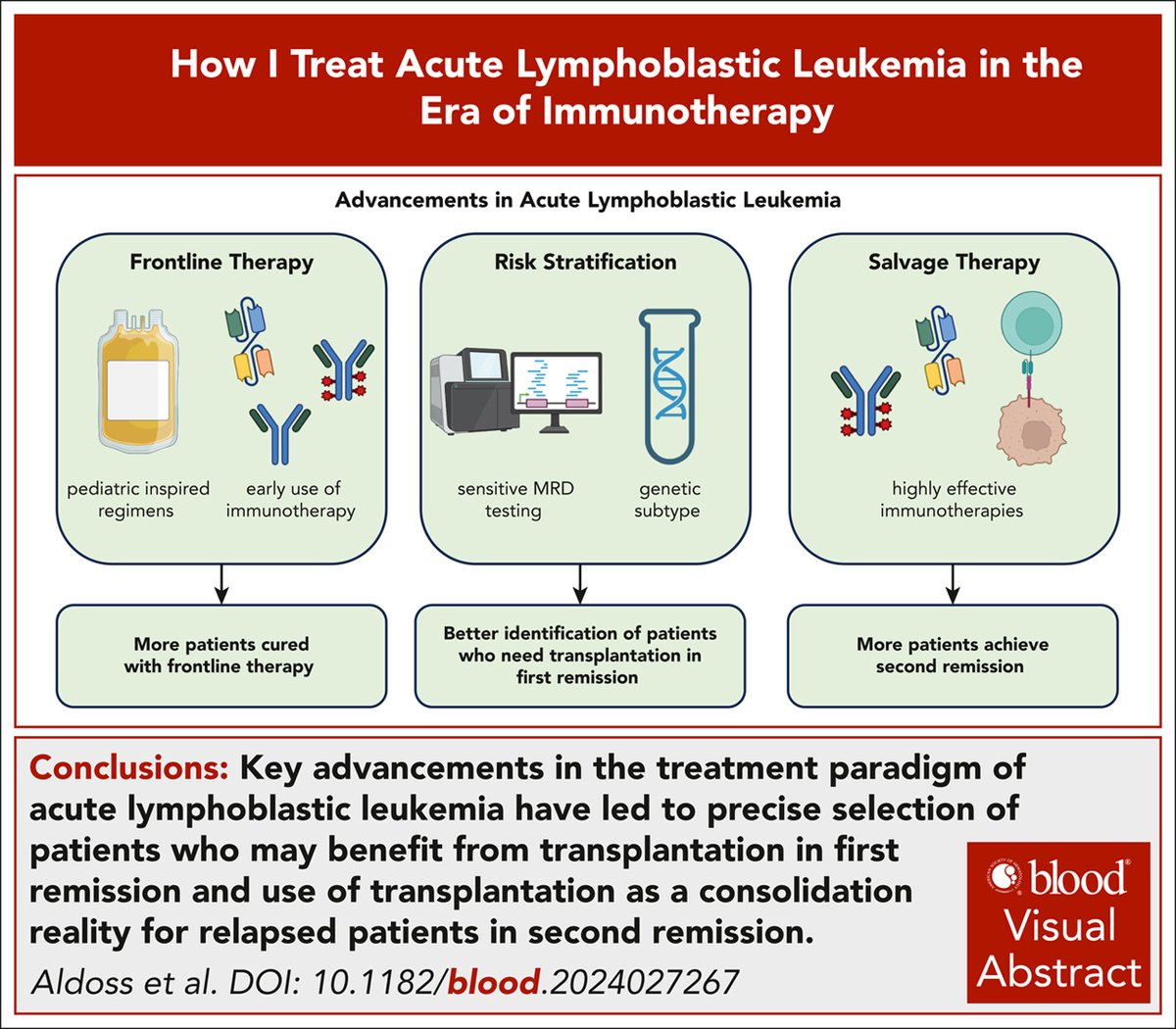
How I treat acute lymphoblastic leukemia in the era of immunotherapy while revisiting the myth of second remission https://t.co/On0MxZygqC #HowITreat#lymphoidneoplasia#transplantation