This game has, without exaggeration, changed my life, my way of thinking. It's taught me about human behavior, our limitations and the desire to always be learning
13 years ago, I wanted to be a part of my favourite childhood game and I'm thankful for those who keep trusting me
Happy Dota Day Everyone!! <3 -- 13 years since full launch, 15 years from open beta, 26 years if you guys are the good ole Dota 1 crowd. OVER A QUARTER OF A CENTURY WITH THIS BEAUTIFUL GAME WE LOVE AND LOVE TO HATE!! #Dota2
I would like to dedicate this win to @GmNaroditsky. It was one of his favourite tournaments. We have played endless bullets and hyperbullets, which definitely contributed to my growth as a player.
Thak gya hoon bol bol kar.
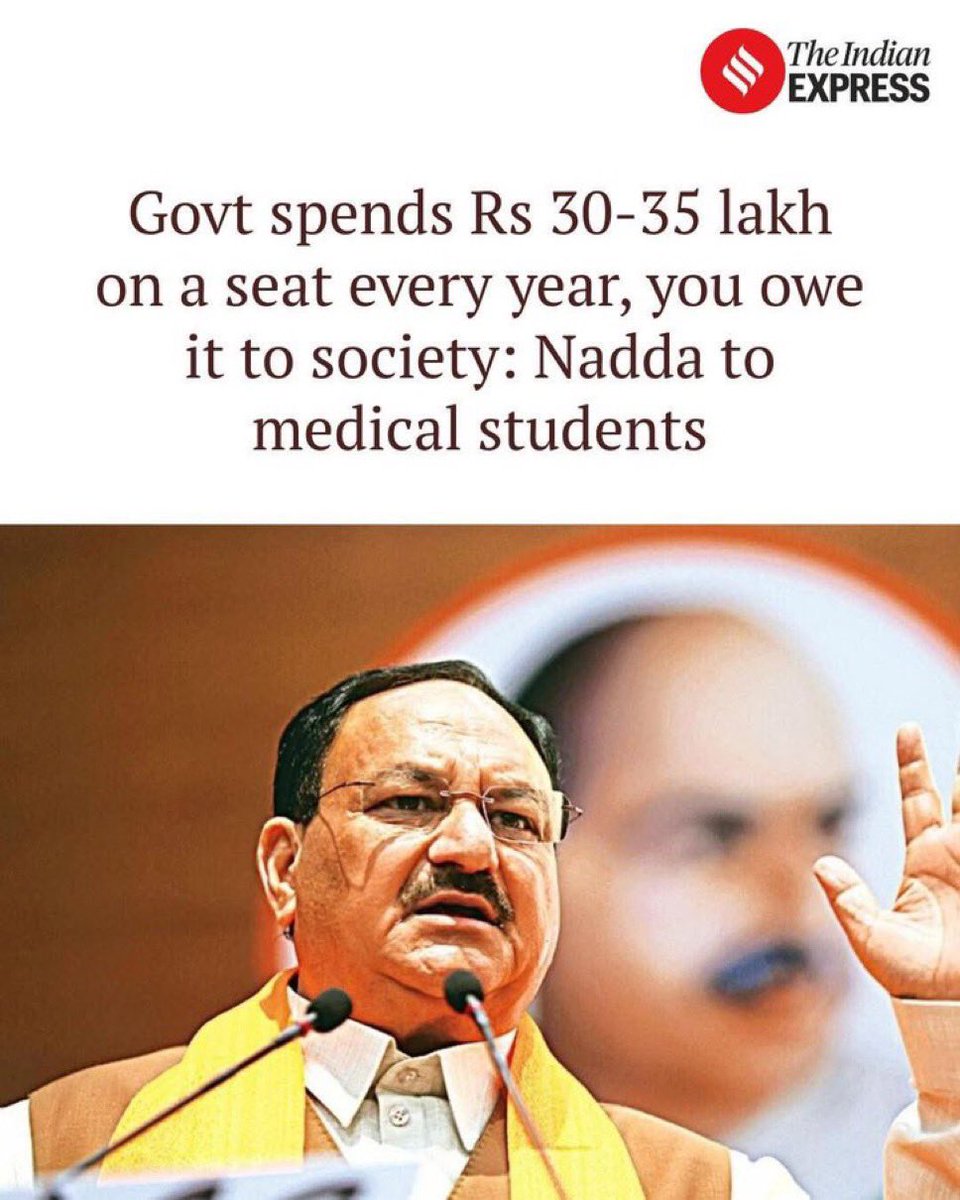
Subsidy is 🔔
AIIMS takes 75000$ for a foreign student. Was 50000$ earlier in 2010s
If anything - the subsidy isn’t more than 30L max.
Or is AIIMS subsidizing even foreign students?
How the fuck did that 1 crore number come up.
It was an internal study published by a professor for his own gain- never even published in a journal - legitimately figment of imagination- given to media - to allow Ramadoss - then health minister to take revenge on AIIMS students for protesting in 2006 Anti reservation protests by not allowing them to go to US citing subsidies etc costs.
Been exactly a year since we launched water purifiers
We now have TDS data from tens of thousands of Atomberg water purifiers installed across the country
And we combined that with publicly available data from different government sources like central pollution control board, jal jeevan mission and central ground water board
And built a free tool where you can enter your pincode and check your water quality- TDS levels, TDS variance, chemicals present etc
Good morning! Just got to know this!
1/2 A whole government Ministry is unleashed on me - because I speak against unscientific practices and primitive traditional healthcare that can harm, I communicate scientific information for public and patients alike.
This was an official memo released during the Ministry of Ayush meeting on 12-6-2026 fully dedicated towards shutting down my social media presence.
Imagine - the people in this meeting were eating biscuits and drinking tea, paid for by the citizens of the country - to decide how to gag and shutdown a citizen doctor who educates people on medical science via social media.
Yesterday, my Instagram account was briefly hacked, but I got back control and removed unauthorized access within an hour.
The Article 51A(h) of the Indian Constitution outlines the fundamental duty of every citizen to develop a "scientific temper, humanism, and the spirit of inquiry and reform". Added during the 42nd Amendment in 1976, this non-justiciable directive promotes logical reasoning, critical thinking, and rationality.
The Ayush system is not scientific, it kills scientific temper, it does not promote the spirit of inquiry, it lacks logical reasoning, has the deadest version of critical thinking and none of its products and practices are rational.
The only thing that needs to be shut down, is an unscientific body like Ayush that goes against the Indian Constitution and wastes public tax money... and not me.
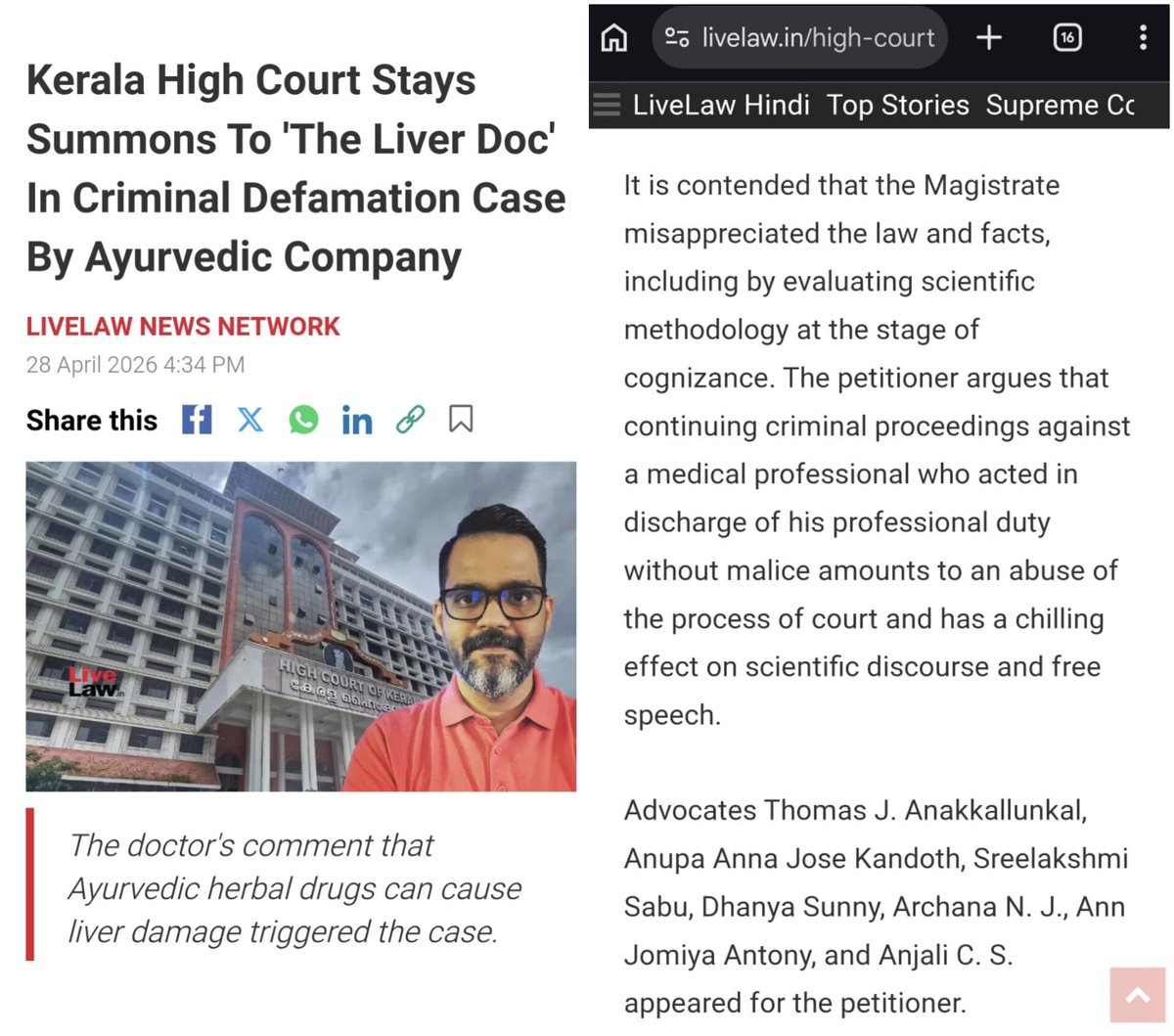
Also, please look closely at the person at the end, who is copied to, by the Ministry. His name is Vaidya K P Manikandan and he is the owner and founder of CNS Ayurveda Hospital, where children are treated for chronic conditions such as severe mental health disorders, autism and epilepsy (please see an official release from the hospital in the next post). One such victim of his was saved by my team (we reported it: https://t.co/eXeWt2n6N7) and he put a criminal defamation case against me and the authors (for publishing a scientific peer reviewed paper!) which was later "stayed" by the High Court of Kerala.
This has nothing to do with service to patients, but everything to do with protecting the business of alternative medicine (especially Ayurveda). These low life complaintants should be ashamed.
Fighting for public against alternative medicine. At what cost? A whole packed outpatient. Sickest patients in the ICU. Non-stop referrals. This whole day was so tough for me. A bit exhausted, but not out.
https://t.co/mhk2pppZvg
An arrest warrant was being planned. Many thanks to my huge team of lawyers in Kochi for fighting this out for me. Not the first, won't be the last. They have been doing this for so long, it takes time, effort, resources and money. This whole ordeal has cost me INR450,000 because the criminal case was tactfully placed in another city.
If you would like to contribute towards the fight for public health against pseudoscience and quackery and help us support our lawyers, please do. We are for the people.
https://t.co/NzvbLRtpSE
Coffee is one of the only drinks with strong evidence that benefits the liver. Here's what decades of research actually says about how to drink it right:
Coffee genuinely lowers liver disease risk.
Meta-analyses show regular drinkers have about 35% lower risk of significant liver fibrosis and nearly 50% lower risk of liver cancer compared with non-drinkers.
Aim for 2–3 cups a day, minimum.
The effect is dose-dependent. The Hepatology socities such as AASLD and EASL says 3 or more cups daily is reasonable for liver benefit, if you tolerate it.
Caffeinated works better than decaf.
But decaf still helps.
Caffeine blocks adenosine receptors that drive liver scarring. Decaf lowers chronic liver disease risk too, just by a smaller margin (UK Biobank, n=494,585).
The target dose: ~300 mg caffeine/day, or 3 cups.
Fibrosis protection kicks in around the 75th percentile of intake, roughly 308 mg caffeine, or 2.25 cup equivalents, per day - the AASLD 2023 advises 3+ cups for liver benefit.
What a "cup" actually means
One standard cup = 240 ml (8 oz), not a 60 ml tiny Indian "cup." A 240 ml filter coffee has ~95–165 mg caffeine. A single espresso shot (30 ml) has only ~60–75 mg.
Coffee-to-water ratio: 1:15 to 1:17.
For filter/drip/pour-over: 15 g of ground coffee to 250 ml water. This is the standard brewing ratio and gives clean extraction of chlorogenic acids and caffeine.
Choose medium roast, not dark.
Medium roast has significantly higher chlorogenic acid (CGAs) content than dark roast. Dark roasting thermally degrades CGAs, the main antioxidant doing liver work.
Arabica beats Robusta.
Arabica beans are richer in CGAs and polyphenols, the antioxidants doing most of the liver-protective work.
A note here:
Arabica for polyphenols, Robusta for caffeine.
Arabica (1.5% caffeine) has more CGAs and polyphenols. Robusta (2.7% caffeine) has more caffeine but a cruder phenolic profile. A 70:30 Arabica-Robusta blend is a reasonable compromise.
Water temperature: 92–96°C.
Just off a rolling boil. Too hot (>96°C) burns the grounds and extracts bitter compounds; too cool (<90°C) under-extracts CGAs and caffeine.
Grind size matters.
Medium grind (table-salt texture) for filter/drip. Coarse for French press. Fine for espresso. Brew time: 3–4 minutes for pour-over, 4 minutes for French press, 25–30 seconds for espresso.
Filtered coffee is the safest daily choice.
Paper filters trap cafestol and kahweol, naturally present plant diterpenes that raise LDL cholesterol if consumed daily in large amounts. Pour-over (V60, Kalita, Melitta) or drip machines with paper filters give you CGAs and caffeine without the cholesterol penalty.
Espresso and French press: fine, but not unlimited.
They retain more polyphenols but also more diterpenes (so more chances of increased lipids). Great occasionally; don't make them your 5-cups-a-day default if you have high cholesterol or heart disease.
South Indian filter coffee: acceptable, with caveats. The metal filter does not remove diterpenes as well as paper, so limit to 1–2 cups/day if you have dyslipidemia. The decoction itself is rich in CGAs. Use less sugar. Skip condensed milk.
BUT ULTIMATE: Drink it black. Or close to it.
Sugar, syrups, flavored creamers and whipped cream cancel the liver benefit, especially if you already have fatty liver, diabetes, or obesity. Skim milk or unsweetened plant milk is fine.
Instant coffee: still works.
UK Biobank (n=494,585) showed instant coffee drinkers had similar reductions in chronic liver disease as ground coffee drinkers. Not as potent, but far better than no coffee.
Cold brew: underrated for the liver.
Medium roast + coarse grind + 6–7 hours at room temperature extracts CGAs and caffeine efficiently with lower bitterness. pH and CGA content are comparable to hot brew.
Timing.
Spread across the day. one at breakfast, one mid-morning, one early afternoon. Stop by 2 pm if you have insomnia.
It helps across almost every major liver disease.
Evidence supports benefit in fatty liver (MASLD), alcohol-related liver disease, hepatitis B and C, cirrhosis, and liver cancer.
The mechanism isn't magic, it's chemistry.
Chlorogenic acid cuts oxidative stress and liver fat. Caffeine inhibits stellate cell activation (that promotes scarring or fibrosis). Melanoidins and polyphenols reduce inflammation.
Who should go easy.
Pregnancy, children, those with uncontrolled heart rate and rhythmn issues (arrhythmias), panic disorder, or insomnia.
And no, coffee does not undo a bad diet or bad choice - such as alcohol, herbal supplement or that Ayurvedic "liver tonic."
Sources: Modi et al., Hepatology 2010; Kennedy et al., BMC Public Health 2021 (UK Biobank); Fuller & Rao, Sci Rep 2017; AASLD MASLD Clinical Care Pathway 2023; EASL 2016 CPG, Frontiers in Nutrition 2026 (Italian coffee cohort).
Hi! I’m currently looking for work opportunities in:
• People Operations / People & Culture
• HR related jobs like HR Coordinator
• Player Manager or Team Manager Assistant (esports) or something similar
I'm happy to connect if you know a position that could fit me, I'm eager to share more. (:
Dear @ICC,
It is with a heavy heart that we now announce our unavailability to replace Pakistan in the upcoming T20 World Cup. Regardless of whether they now withdraw, the short timescales ensure it is impossible for our squad to prepare in the professional manner necessary to compete effectively in this global cricketing spectacle. We are not like Scotland and able to turn up on a whim, with no kit sponsor.
Our players are from all walks of life and cannot simply drop their occupations to fly halfway around the world to experience temperatures only normally felt in Finnish saunas. Our captain, a professional baker, needs to attend to his oven, our ship captain needs to steer his vessel, and our bankers need to go bankrupt (again). This is the harsh reality of cricket at the amateur level of the game.
This news will be extremely disappointing to our fans. Despite being the most peaceful nation on Earth, we maintain an army of online followers, and are the world's 14th most followed national board on X. We were ready to give the Dutch the biggest shock they have experienced since William of Orange lost the Battle of Landen in 1693. And the Americans were looking forward to taking on Greenland, or so their orange-dyed leader thought.
Our loss is likely Uganda's gain. We wish them well. Their kits cannot be missed unless you have epilepsy, in which case they are probably best avoided.
The future is always ice, until it isn't.
Yours sincerely,
Icelandic Cricket Association
Confidential sources report that during a 6-minute halt in the badminton match caused by a pigeon pooping on the court, both the Indian and Singaporean players ordered ORS juice through Blinkit and paid seamlessly via UPI. If this isn't peak development, then what is?
STAY WITH ME.
A few years ago, a patient was referred to me because he was diagnosed with complicated cirrhosis. He had an infection which led to a condition called hepatic encephalopathy (brain failure due to high ammonia levels). The treatment largely involved ammonia reducing therapies. One drug was central to this - Rifaximin - a non-absorbable antibiotic that reduced ammonia in the body. I prescribed him Rifaximin for 6 weeks and advised him follow-up.
He came back to me, not after six weeks, but in 4 weeks, this time, in liver coma (worst stage of brain failure - due to very high ammonia). He spent two days in the ICU and six days in total in the hospital. His hospital bill was close to INR 80,000. He had no insurance and his wife borrowed the money from neighbors and friends to clear hospital dues.
Upon questioning, I found that he was not taking the Rifaximin drug I had prescribed. He was only on the other two drugs (one, a syrup called lactulose for improving ammonia clearance in gut). I was furious, because the patient spent a whole week unecessarily in the ICU and wasted so much money that he never had - just because he was "not compliant" to my orders. I decided it was time for me to school him a bit.
But I was wrong. He was compliant. He had purchased Rifaximin and was on it. For 15 days. Thereafter, he could not afford it. He was an autorickshaw driver who shuttled school children every morning and evening. He could hardly make ends meet. He had two children of his own. The Rifaximin brand I prescribed him was 42 rupees per tablet. He had to consume two a day - which would mean 2520 rupees a month. He just did not have that money - so he skipped it - to not compromise on other important matters - childrens education and food.
He was confused and scared about opting for a cheaper version of Rifaximin because one, he was unsure about the quality of Rifaximin that was not prescribed by me and two, he was "scared" that I would scold him for buying a cheaper Rifaximin and if that got him into trouble.
I was confused and scared about prescribing a cheaper version of Rifaximin because one, I was unsure about the quality of Rifaximin that was not "a good promoted brand" and two, I was "scared" that his family would scold me for prescribing a cheaper Rifaximin and if that got him into trouble.
It is heartbreaking that many doctors still simply don’t trust generic medicines. Too often, they worry that these cheaper options are lower quality or might cause more problems than the big, famous brands. This fear leads them to prescribe expensive drugs instead, and the real tragedy is that it pushes vital healthcare out of reach for the ordinary people who need it most - like my patient.
This narrative, that generic drugs 'are never good' and that only big pharmaceutical marketed drugs are what works has been deeply ingrained into doctors and patients alike - I do not know by whom and since when. Looking back, these strong emotions were based on either opinions, testimonials or second- and third-hand information. Not evidence.
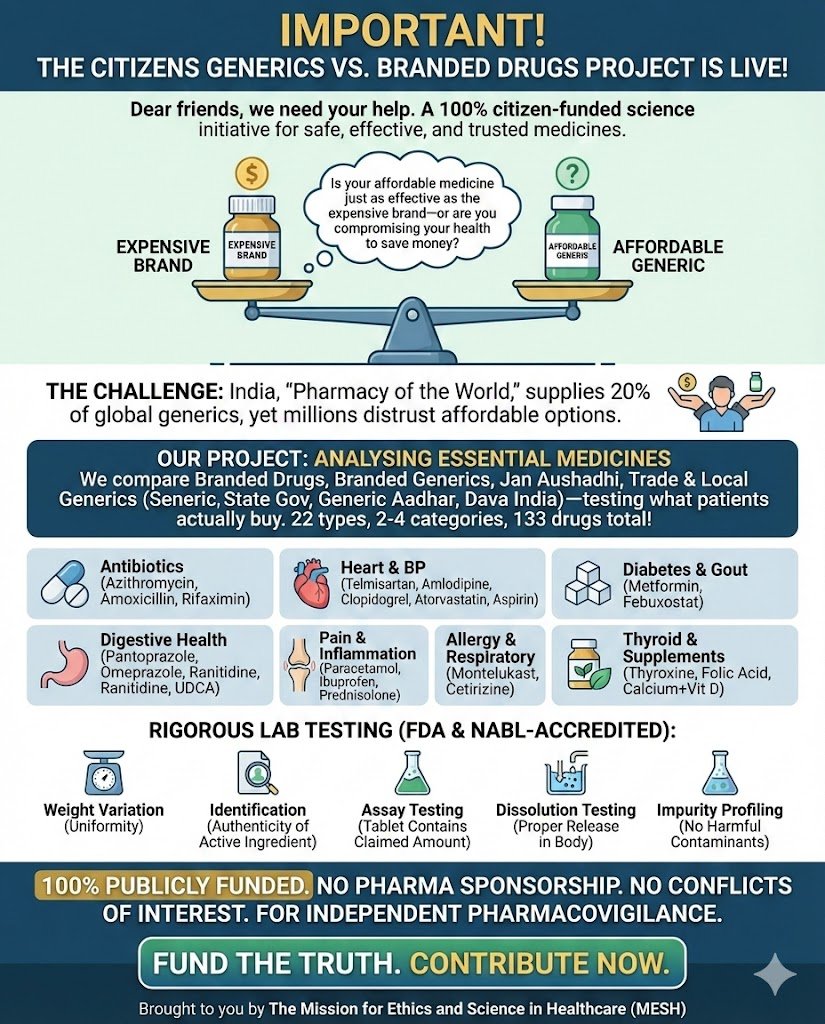
Like I said. Stay with me. This is life changing and will disrupt the drug market in India. Here are the results of The Citizens Generic vs. Brand Drugs Quality Project.
1/11
I don’t want bonds for either IIT/IIM and no bonds for doctors too. My position isn’t bonds for engineers but no bonds for docs
If you IITian justify that you don’t deserve Bond but doctors do-then congrats- you’re a hypocrite wanting capitalism for thyself/socialism for others.
How much unpaid labour does a resident do.
A resident salary- give or take is around 1 Lakh/month.
Residents are supposed to work 50hr/week.
So, 200 hr/month = 1 Lakh.
So, basically 500₹/hour.
How much a Resident works?
On an average 80-90 hours - so approximately 40 hours per week and 160 hours extra in a month.
Overtime is supposed to be twice of normal but Ill use only 1.25X since we ‘owe’ to govt.
So, on an average 160hours/month * 500₹/hr *1.2x
= 1 Lakh worth of unpaid labour.
So for JRship - it was 36L worth of unalie labour.
Add 3 year of DM/SRship. (Pay is higher but I’ll consider same)
Total amount owed to doctors- 72Lakh.
Doctors don’t owe shit to govt.
You make back everything in unpaid labour and more.
This fucking lie.
No, you don’t spend anything on us.
The hospital exists independent of college.
AIIMS was created a hospital - not just for MBBS. Institutes like PGI don’t even have MBBS.
You can’t take health budget and divide by number of MBBS students and say we spend that much.
The budget for academics is 10% of entire budget of hospital.
If you spend - it’s 3-5L, not 30L/year.
And most govt colleges now already have 2-3L fees.
There is zero subsidy.
>> https://t.co/SKdsWZL3U7
OKAY, practicing doing scripted content. A prior Bridges guest, Stephanie Lepp, invited me to create a video outlining and integrating different perspectives on free speech. This is part of her 'Faces of X' series, which seeks to articulate a ✨synthesis✨ on complex social issues. Share your thoughts, and maybe I'll do the J6 video next. (:
Generic drugs vs. Branded drugs project
An update.
Within 24 hours, we were able to raise ₹1200,000/- with you kind support. This is massive - a sign of great interest from the public. Help us keep it alive.
The whole project cost is ₹2793000/- including detailed analysis work, purchase, transportation, logistics, future paper publication and open access fees.
We do not have any sponsors other than you.
Please help us reach the goal so that this project sees the light at the end of the tunnel. There is no other major public health project that is so important in India right now. And you can help us go the distance.
To contribute, please go here: https://t.co/6YXy2Ko6hT - and share this with your family and friends.
If you have entrepreneurs or business owners who are interested in not-for-profit healthcare projects like these and would like to contribute larger sums to this public health project, please get in touch with them too with the link and project details. We want to kick-off the analyses early next week.