Stop press: sterile gowns are no longer mandatory for spinal anaesthesia.
I’m so proud to have been part of this process trying to simplify our practice, making us more efficient, more sustainable without increasing risk to our patients.
https://t.co/JxQoNmkBql
Professor Harold Ellis died yesterday aged 100.
Fond memories of undergraduate anatomy at @Cambridge_Uni an inspiration and mentor to generations of doctors
May he rest in peace
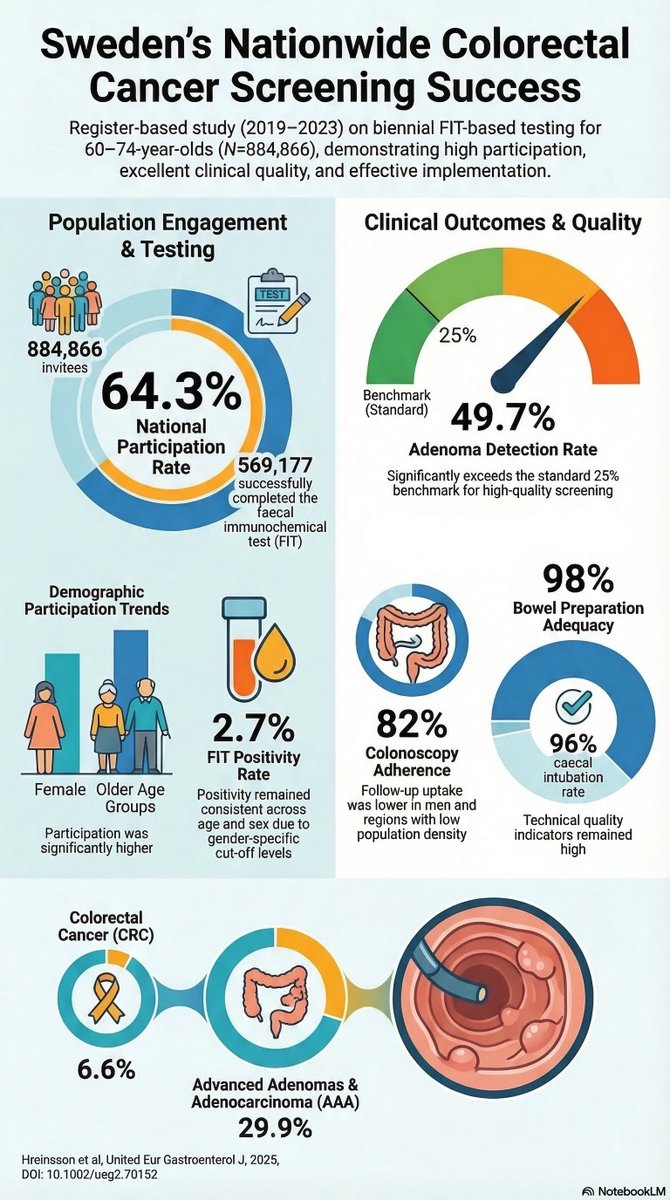
In 2019, Sweden rolled out their national FIT-based colorectal cancer screening programme to those aged 60-74.
This @UEGJournal study presents the first 5-year data of their screening programme.
#ColorectalCancerAwarenessMonth
📸: https://t.co/PGmjOBm4u7
Makes the blood boil.😠
'more female surgeons experienced pregnancy complications compared with female partners of male surgeons, but this difference did not persist after accounting for lack of workplace support.'
It's PREVENTABLE. #GenderBias#wellbeing
https://t.co/XZ3emxBkuT
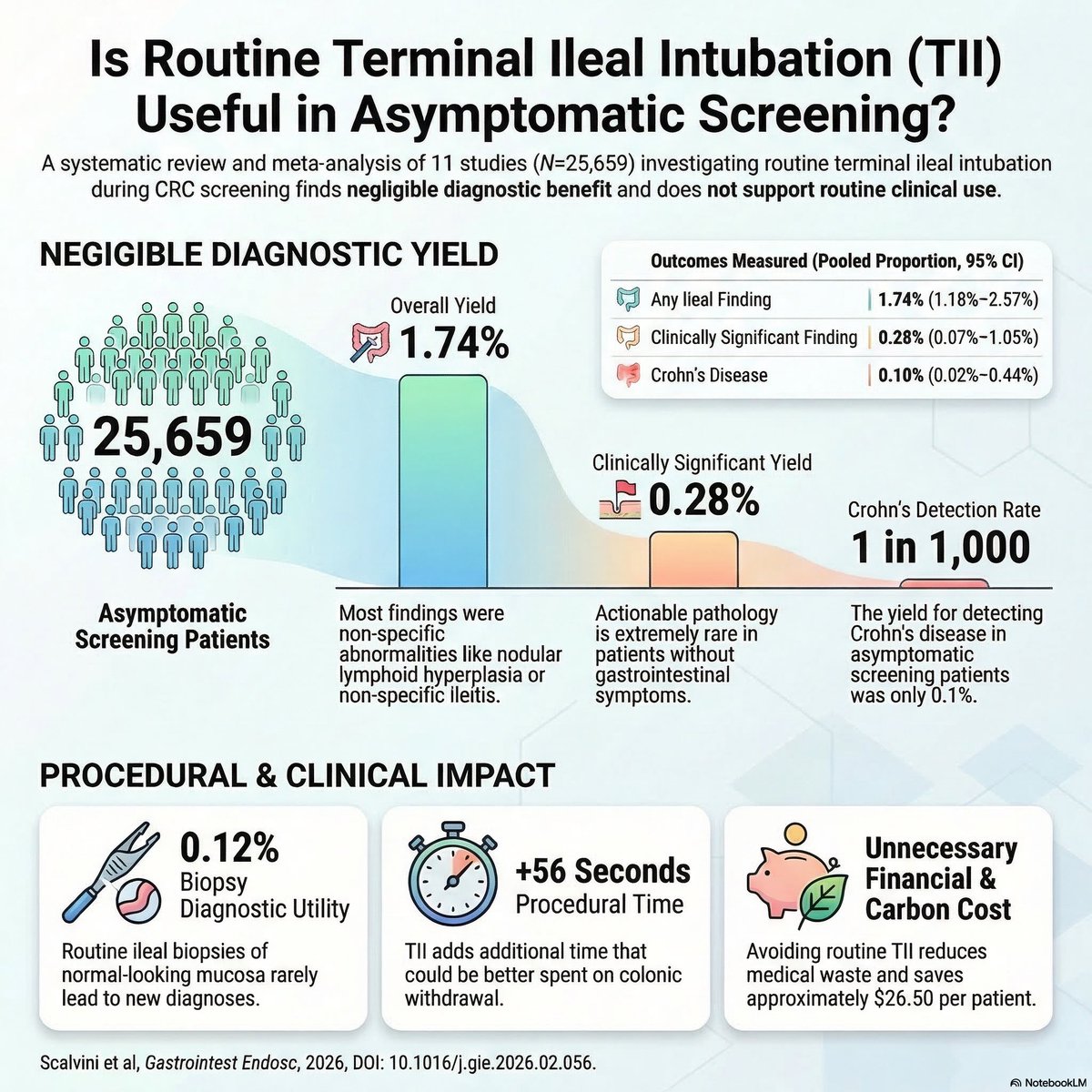
🤔 Should we be doing routine terminal ileal intubation during colorectal cancer screening colonoscopy? 🔦
💡 No, according to the results of a newly published meta-analysis 👇
Ileocaecal resection versus infliximab for ileal Crohn's disease: retrospective 10-year follow-up of the LIR!C trial - The Lancet Gastroenterology & Hepatology https://t.co/OBIMkVWTu8
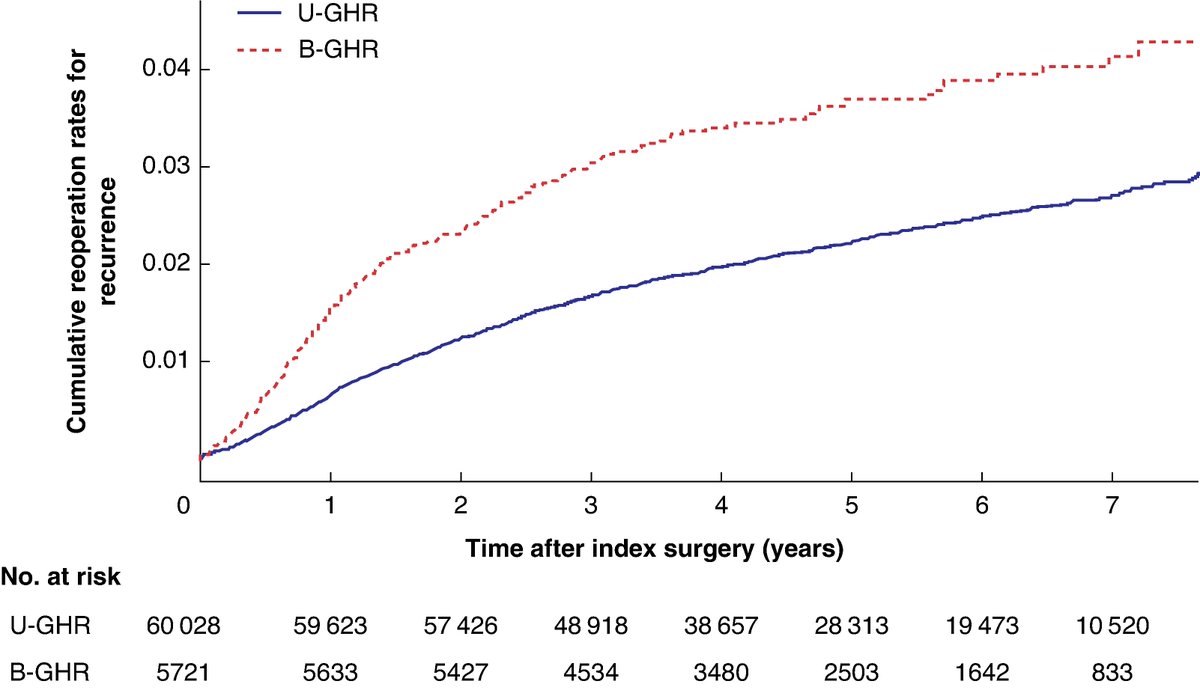
Recurrence and patient reported outcomes after simultaneous bilateral versus unilateral groin hernia repair: prospective nationwide cohort study
➡️https://t.co/GZ9ruVXJ63
This large-scaled nationwide cohort study including both sexes found a significantly higher associated risk of both chronic pain and patient dissatisfaction 1 year after bilateral compared with unilateral groin hernia repair. Women and younger patients are particularly at risk, suggesting a more cautious approach to simultaneous bilateral groin hernia repair in routine practice, especially in the absence of clear symptoms, and highlighting the importance of watchful waiting.
👏👏👏Ramia Stolt , Hanna de la Croix , Henrik Holmberg , Maria Melkemichel , Agneta Montgomery , Benedit Witermark , Pär Nordin
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @BJSAcademy@BJSurgery@eurohernias #hernia #hernia @herniaistanbul@BritishHernia@HerniaIndia@awrsurgeons
Systematic review and meta-analysis: Prophylactic TXA use was associated with lower intraoperative blood loss, transfusion requirements, and major bleeding without an observed increase in thromboembolic or mortality risk. https://t.co/1zvzFHQb7e
The @RCSEdFST@asmeofficial grant funded #SuperDuper study is still recruiting
We are looking for surgical/obstetric trainees ST1-5 - get some free coaching on performance enhancing routines and help us understand if they can increase #surgeon#performance
Link below...
A lot of people in academic medicine explain things in an overcomplicated fashion, in part to create a certain mystique around themselves and give others the impression that they understand things at some higher level than the average practitioner is able to.
It works especially well if the person sounds confident when they speak, because the listener will usually not have enough mastery of the subject to question them on it. People think that when they can’t understand what’s being said, that the problem is with themselves. Entire careers are built on this dynamic.
As learners, you have to recognize that this behavior is often false. True geniuses do exist, but are rare. The prevalence of individuals that truly understand things that no one else can is definitely much less than 1 per department.
The 2 take-home messages from this are:
1) In general you want your teachers to spend most of the time making things reductive; in other words, making them seem simpler, not more complex.
2) the confidence with which someone says a thing has little correlation to whether it is true or not. Being a good salesperson helps one’s career in medicine as much as it does in other fields, and you have to recognize when the person talking to you is bluffing.
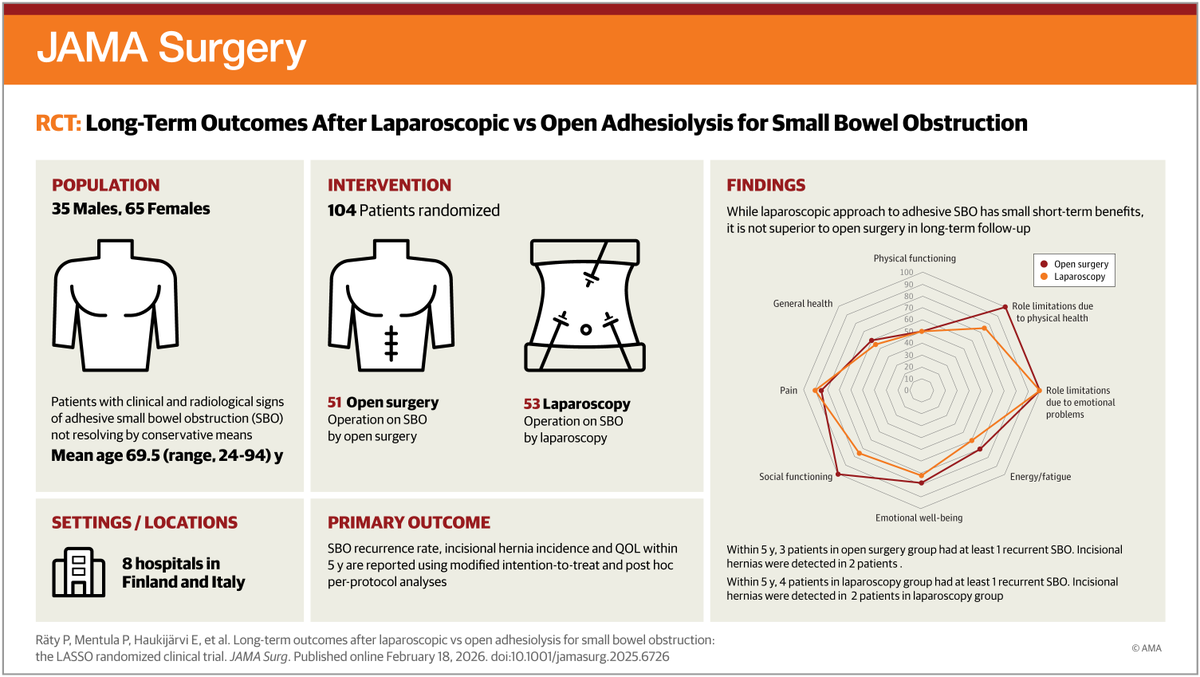
Laparoscopic adhesiolysis for #SmallBowelObstruction was not superior to open surgery for long-term recurrence, incisional hernia incidence, or quality of life at 5-year follow-up, confirming both as viable options.
https://t.co/QXd9BgLfEQ
Semaglutide, fasting and gastric ultrasound
Nearly 50% of patients receiving semaglutide treatment had a full stomach on pre-operative gastric ultrasound, regardless of dose, duration, route of administration or withholding time.
#anaesthesia#MedTwitter
https://t.co/BikU3cDeUL
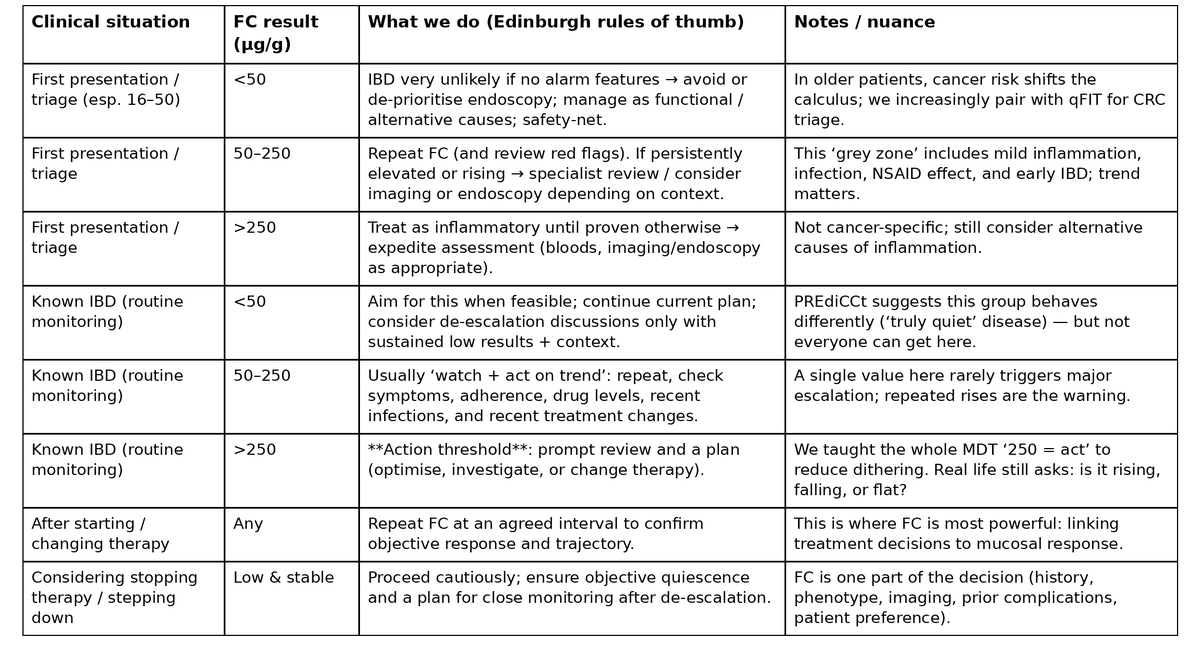
How do you actually act on a faecal calprotectin result?
We've been refining this in Edinburgh for 20 years.
Here are the three tables from the new Atomic IBD post; starting with the one you can use in clinic tomorrow.
"Monitor, monitor, monitor ... and act on the results of the monitoring."
Different clinical situations need different responses.
• First presentation isn't the same as routine monitoring.
• "Grey zone" results need context.
• And the 250 threshold is a decision point, not a diagnosis.
We taught this to everyone: doctors, nurses, pharmacists, administrators even surgeons.
#Cholecystectomy for acute gallbladder disease showed similar bile duct injury rates with robotic-assisted vs laparoscopic methods, but robotic-assisted use was linked to more major complications & longer hospital stays.
📽️ Watch the video & learn more: https://t.co/9lCF3pfdm6
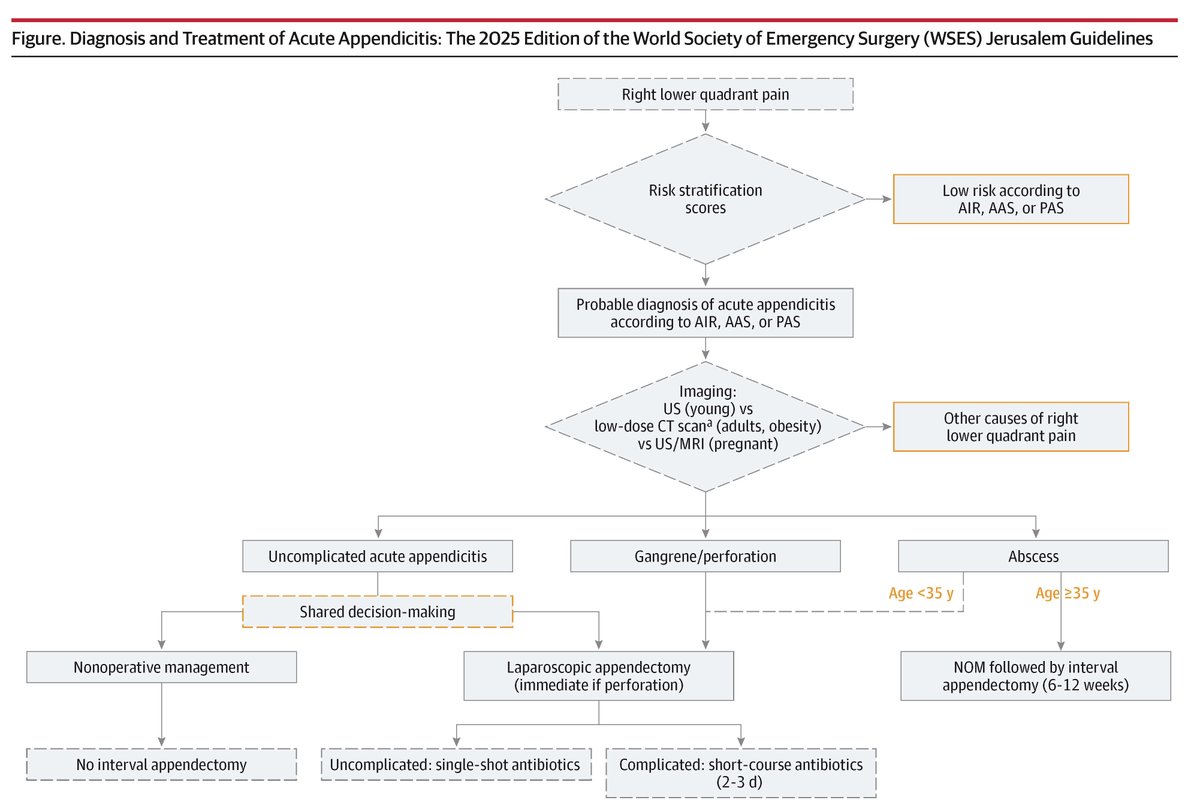
The 2025 WSES #Appendicitis guidelines recommend risk stratification and imaging for diagnosis, outpatient antibiotics for uncomplicated cases, and laparoscopic surgery within 24 hours for surgical management.
https://t.co/DHDQLShgPy
A sex bias in the decision about which surgical cases to postpone or cancel may contribute to compensation inequality in a fee-for-service setting. https://t.co/4lZC3NGM5U
Most surgeons do not modify their workload during pregnancy, potentially contributing to feeling overworked and peri-partum complications. https://t.co/CRuP9nXjba