In a new blog post, Dr. Michelle Kittleson writes that clinical decisions should be driven by the patient’s medical needs, not by physician concerns about their status, expectations, or perceptions.
Read “Very Important Patients”: https://t.co/7hsjVnY53s
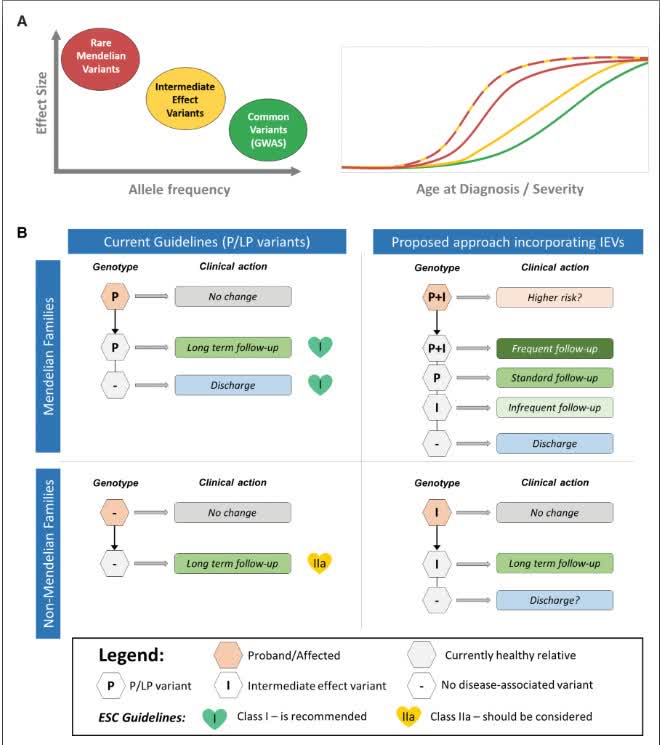
Intermediate effect variants (IEVs) in HCM genes are routinely misclassified as variants of uncertain significance, yet carry odds ratios of 5-15 and are found in 6% of HCM cases vs. 1% of controls. Proposed framework on how to incorporate into practice. https://t.co/cqpriDzNyv
ATTR is often found in the tenosynovium & transverse carpal ligament in older pts with carpal tunnel syndrome; >25% have #ATTR cardiac amyloid detectable by bone scintigraphy. Biopsies at carpal tunnel surgery may enable earlier #ATTRCM Dx & Tx. https://t.co/idkODjNjHq #JACCHF
🧬 LMNA cardiomyopathy: not all patients progress the same.
Now we can quantify who will.
We’ve become good at predicting:
👉 sudden death
👉 arrhythmic risk
But heart failure?
👉 Still a blind spot in laminopathies
💥 This paper changes that.
For the first time:
👉 a dedicated risk model for HF progression in LMNA patients
📊 The reality (and it’s not reassuring):
• HF-MACE in ~10% at 5 years
• ~45% lifetime risk by age 70
And if LVEF <30%:
👉 50% events within 1 year
ehag104
⚡ Four variables. That’s it.
Independent predictors of HF progression:
• Male sex
• LVEF <50%
• Missense variants (head/rod domains)
• Complete LBBB
🔥 Translation:
👉 Genetics + conduction + early LV dysfunction
= the HF trajectory is already written
📉 What’s really striking (Figure 4):
• 0 risk factors → ~1.5% at 5 years
• 1 factor → ~5%
• ≥2 factors → ~22%
➡️ Not a spectrum
➡️ A stepwise risk escalation
🧠 And here’s the key insight:
👉 Even with preserved EF, risk is not low
Patients with LVEF ≥50% + risk factors:
→ still meaningful HF risk (~11% at 5 years)
ehag104
⚠️ This challenges our mindset:
We wait for EF to drop
👉 But the disease is already progressing
💡 Clinical implication (this is the real shift):
Risk stratification in LMNA should not be:
❌ reactive
❌ EF-driven
But:
👉 proactive + genotype-informed
🚀 What this enables:
• Earlier follow-up intensification
• Earlier HF therapy
• Earlier referral for advanced HF pathways
• Better selection for trials
🎯 Take-home message
LMNA cardiomyopathy is predictable.
👉 Not just arrhythmias
👉 Heart failure too
And if we wait for severe dysfunction…
👉 we are already late
💬 Should we start treating LMNA patients before EF declines?
#Cardiology #LMNA #Cardiomyopathy
#HeartFailure #Genetics
#PrecisionMedicine #EPeeps #CardioTwitter 🧬🫀
https://t.co/KTBgHlKM5W
🎇 🔥 Exciting breaking news! 🔥 🎇
NEJM Voices features essays grounded in real-world practice -- including pieces by me (!!) that will appear every 2 weeks.
Check out my inaugural essay, about how a country-music star made me a better doctor. I hope you like it 😊
In a new blog post, Michelle Kittleson, MD, PhD, explains how a patient’s reference to a late-70s country hit inspires a framework for shared decision-making. Read “Kenny Rogers and the Art of Shared Decision-Making”: https://t.co/xkUz5CMCY1
💥Practice-changing #FLECA-ED data at #EHRA26!
In patients with paroxysmal AF + CAD (no residual ischemia), IV flecainide blew away IV amiodarone: 85.7% vs 40% successful cardioversion to sinus rhythm at 6 h (p<0.001), median time 20 vs 244 min, identical safety (no VT/NSVT at 24 h).
In my practice, I routinely use short-term flecainide (pill-in-the-pocket at home or in the hospital) in stable CAD patients if acute ischemia is excluded. Yet real-world practice still varies wildly - do we really need to fully rule out ischemia before even a single dose?
My friends @AndrewJSauer and @MichaelNassifMD may disagree, but to me, the pendulum has swung too far against IC agents after CAST. This trial supports re-evaluation for acute use in CAD without residual ischemia.
Great work @ptsioufis & team!💪
Comprehensive evaluation of hypertrophic cardiomyopathy: European Journal of Heart Failure expert consensus document
Establishing the correct diagnosis, which requires differentiation between sarcomeric HCM and phenocopies such as amyloidosis, Fabry, or mitochondrial disease, using multimodal imaging and genetic testing. (ii) Establish presence of symptoms and of left ventricular outflow tract obstruction (LVOTO), which is central to symptom evaluation, prognostication, and treatment
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@HFA_President@EJHFEiC@ESC_Journals@DrMarthaGulati@hvanspall@ShelleyZieroth@dranulala@Hragy@cardioceptor
https://t.co/HTcHF50Zfh
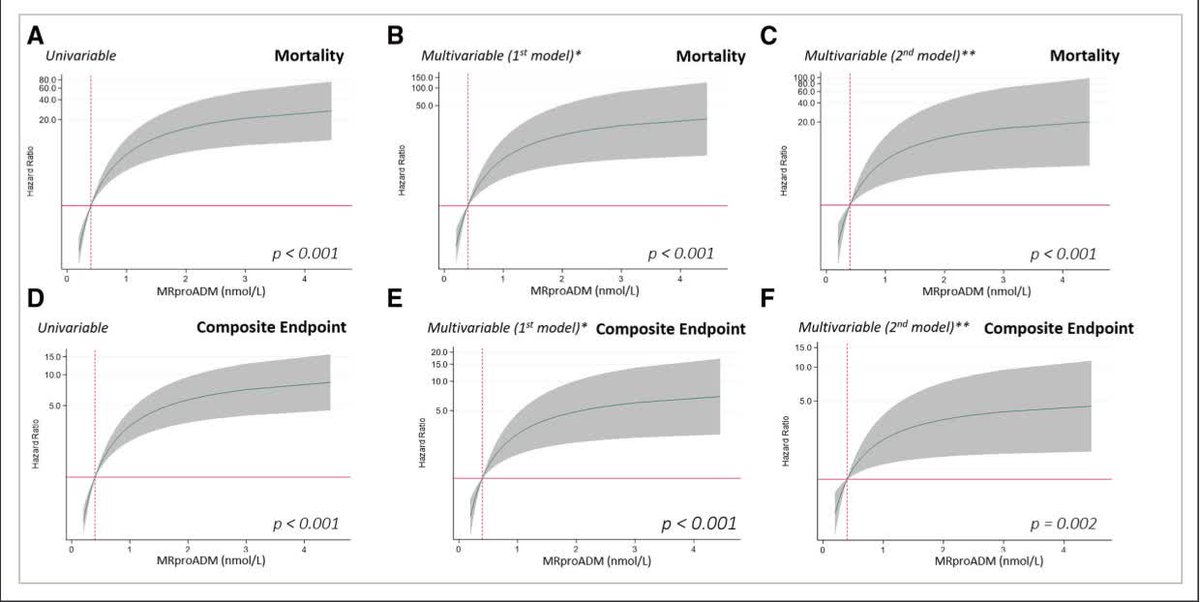
Accurate prognostication remains an unmet need in ATTR #amyloidosis. In this brilliant work by @peiro_belen et al., MR-proADM emerges as a strong predictor of outcomes, improving the performance of current staging systems such as NAC and Columbia.
Proud of being part of the team!
🚀 Hypertrophic cardiomyopathy: from a feared disease to a treatable condition
I’m excited to share this outstanding review highlighting how hypertrophic cardiomyopathy (HCM) has dramatically evolved over the past decades.
💡 Why this matters
Once considered a rare disease with a poor prognosis and high mortality, HCM is now recognized as a common, manageable condition with near-normal life expectancy.
🔬 Key takeaways:
📉 A remarkable reduction in mortality
✔️ Historical mortality ≥6% per year
✔️ Today → ≤0.5% per year in optimally treated patients
✔️ Comparable to the general population
👉 A true transformation in cardiovascular medicine.
🫀 What changed the natural history?
⚡ Prevention of sudden cardiac death
✔️ Implantable cardioverter-defibrillators (ICDs)
✔️ Highly effective risk stratification (~95% sensitivity)
💉 Stroke prevention
✔️ Early and aggressive anticoagulation in atrial fibrillation
✔️ >3-fold reduction in embolic events
🔧 Reversal of heart failure
✔️ Surgical myectomy → symptom relief in >90%
✔️ Improved survival and quality of life
✔️ Alcohol septal ablation as alternative in selected patients
💊 A new pharmacological era
✔️ Cardiac myosin inhibitors (mavacamten, aficamten)
✔️ Targeting disease mechanism → improving symptoms and gradients
🧬 Precision medicine in action
✔️ Genetic understanding (sarcomere mutations)
✔️ Family screening and personalised management
✔️ Dedicated HCM centres driving expertise and outcomes
🌍 A paradigm shift
HCM is no longer a “high-risk” disease:
👉 Most patients now achieve normal or near-normal longevity
👉 Severe outcomes are largely limited to a small subset with advanced disease
🫀 A powerful reminder of what modern cardiology can achieve:
From fatal to manageable — through decades of research, innovation, and patient-centred care.
👏 Congratulations to all the pioneers who transformed the HCM landscape.
#Cardiology #HCM #HypertrophicCardiomyopathy #PrecisionMedicine #HeartFailure #SuddenCardiacDeath #Innovation #MedTwitter #CardioTwitter #Research
https://t.co/VhrWd9HJCc
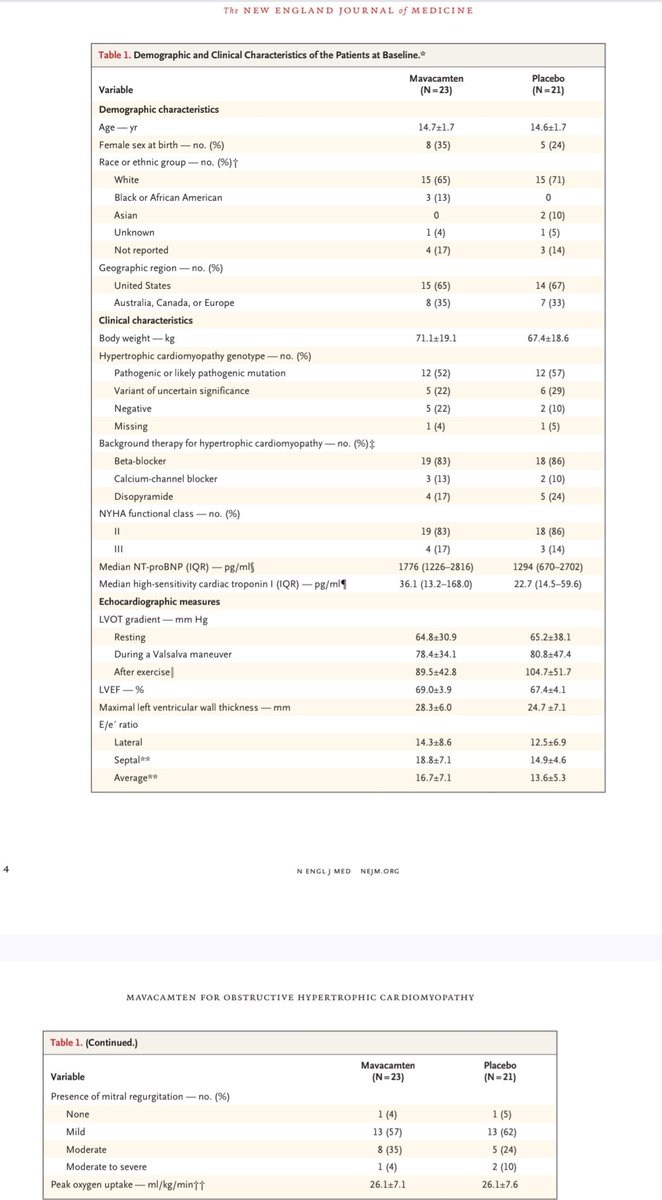
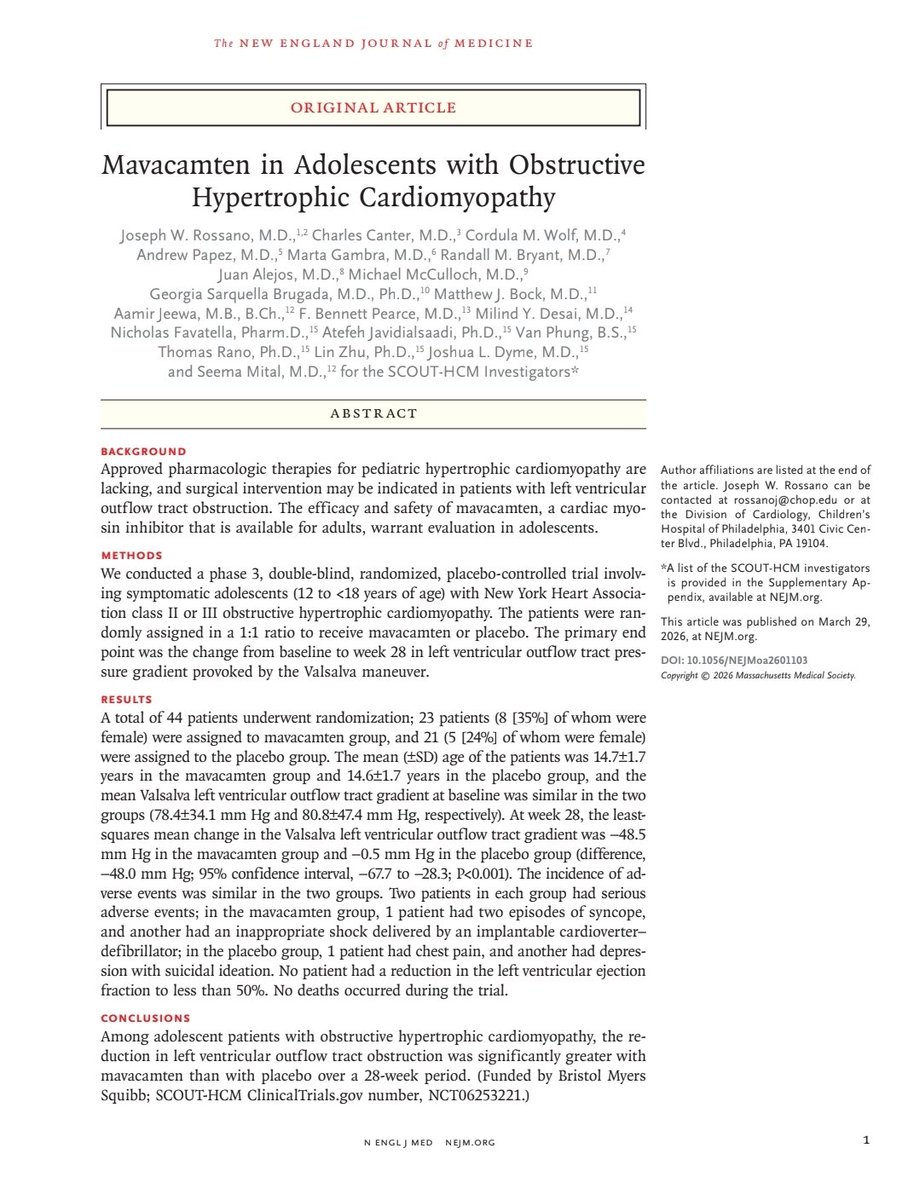
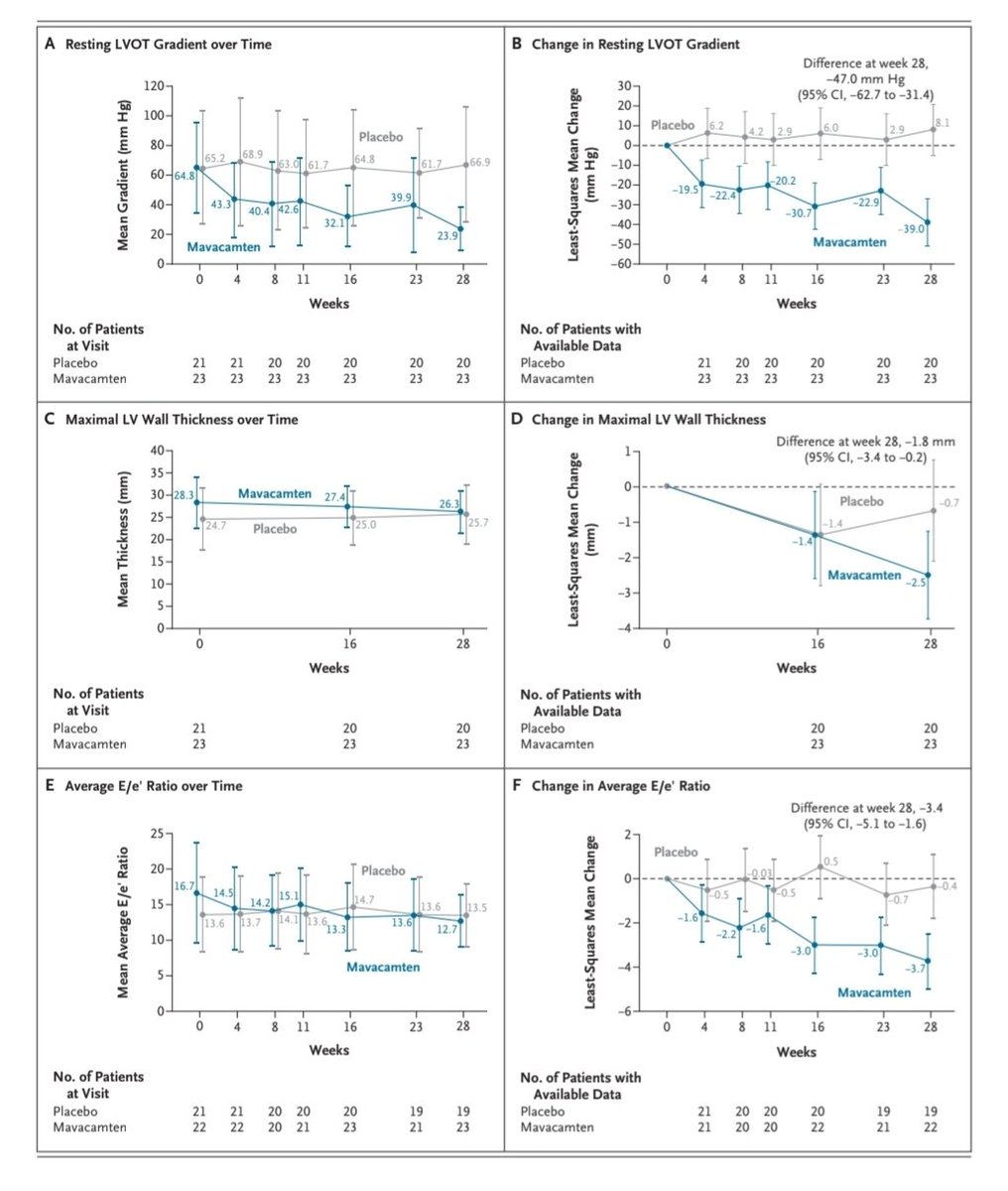
#ACC26 Mavacamten in adolescents with obstructive HCM. Results from SCOUT-HCM
Overall consistent with what was seen in adults. Requiring higher doses of drug. Small sample size but reassuring safety that isnt expected to diverge much from what was observed in adult trials (potentially even safer due to shorter disease duration, less comorbidities, less restrictive disease)
https://t.co/psIlV32nWZ
#CardioTwitter
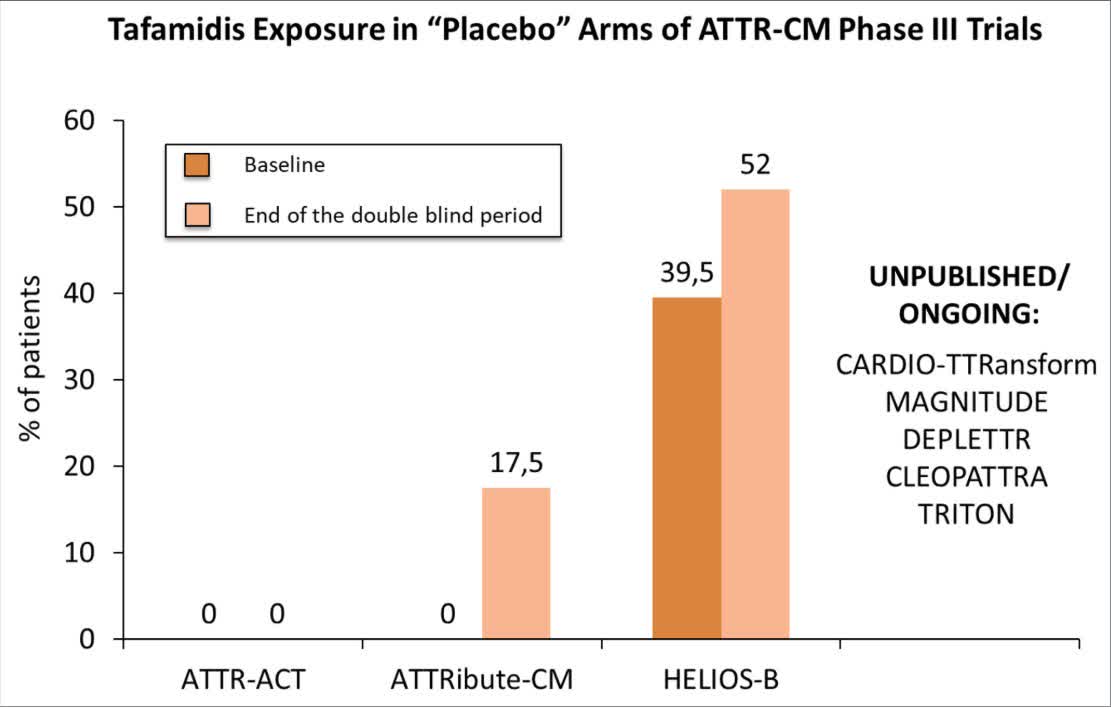
#OnMyMind: In transthyretin amyloid cardiomyopathy (ATTR-CM) trials placebo arms are often poorly controlled; urge standard of care-anchored designs with anti-amyloid therapy.https://t.co/ogLQhdTzUj