Seeing a straightforward patient - 3min. Paperwork & process around seeing the patient, 15min. Interruptions while dealing with paperwork & process, +30min. 45 min for a patient that spends 3 min with me. I’m not value for money. Reminds me of this paper. https://t.co/sDCrBzTTeH
Fragmented systems - often contributed to by the passionate people who set up amazing Pre-Hospital services - Founders Syndrome - be able to identify when 'your baby' needs to be in someone else's hands
- Michael Dickson
@_retrieval#retrieval2025
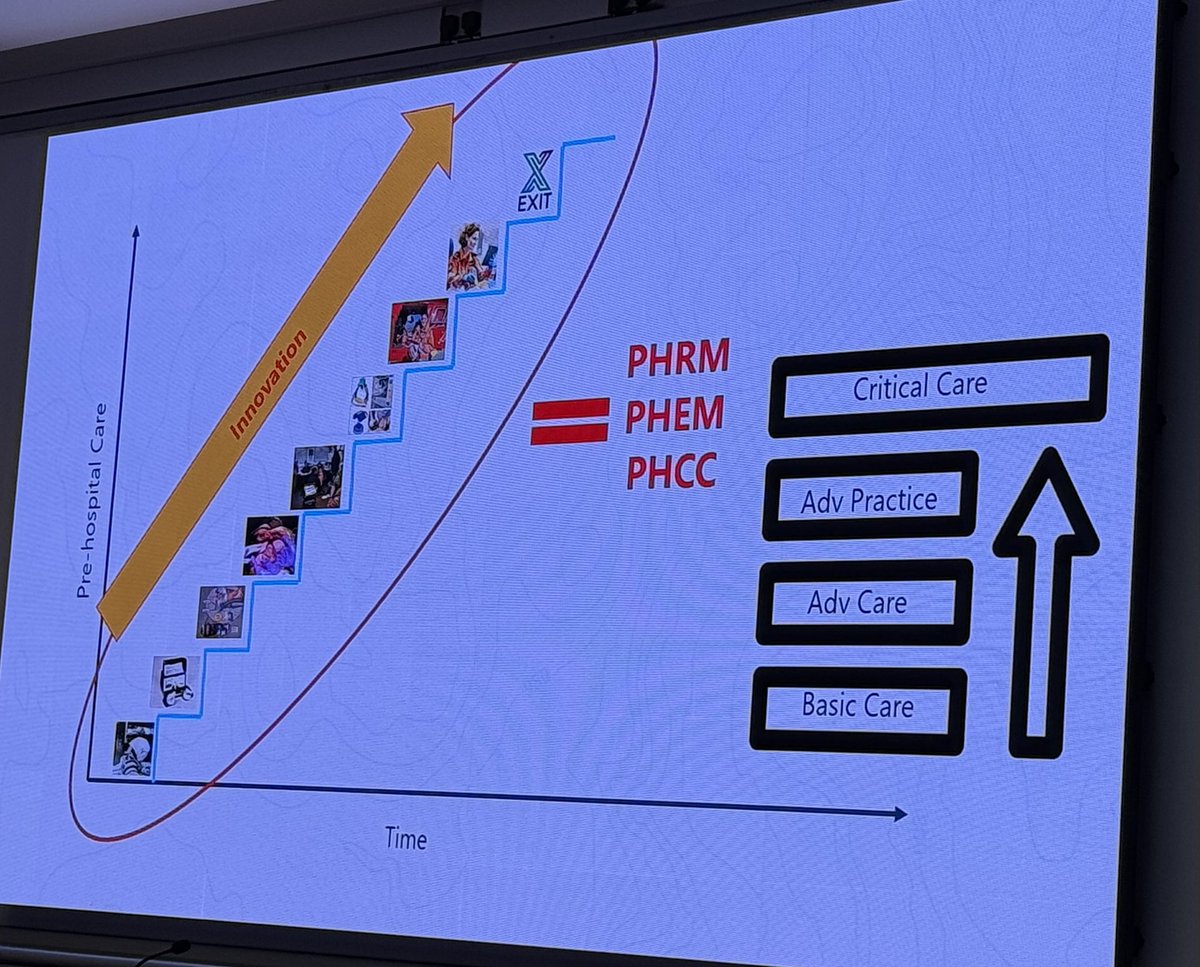
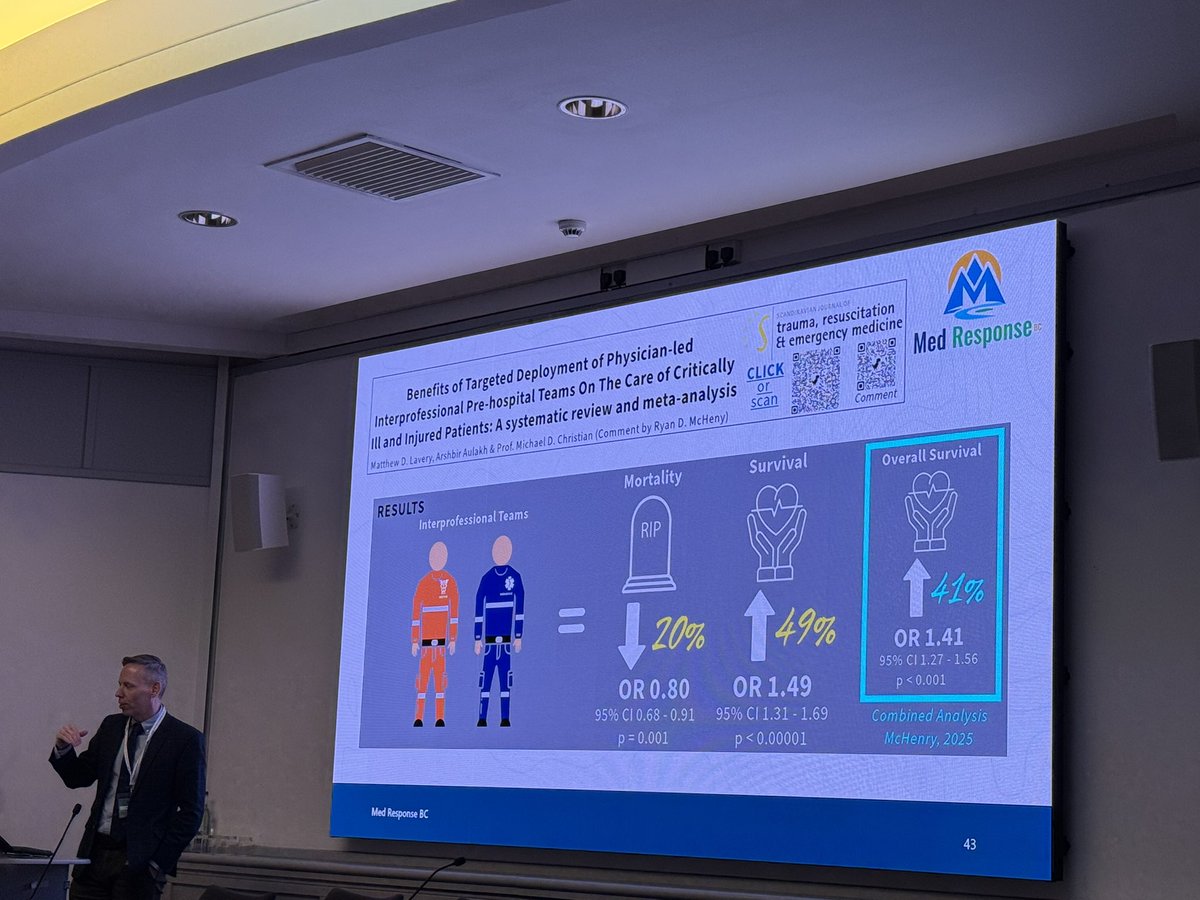
Perception by some that 'Critical Care' is a defined set of knowledge / skills to be taught & delivered but 'Today's Critical Care is Tomorrow's Advanced Care' - Prof Mike Christian @_retrieval#retrieval2025
ICU Line Secrets:
Is there anything about "lines" that has not been done or studied already? Not much, I guess, so these actually are not secrets, just things I had to do the last couple of weeks & hopefully you also find useful in your practice
Here it begins:
1. "Twin lines"
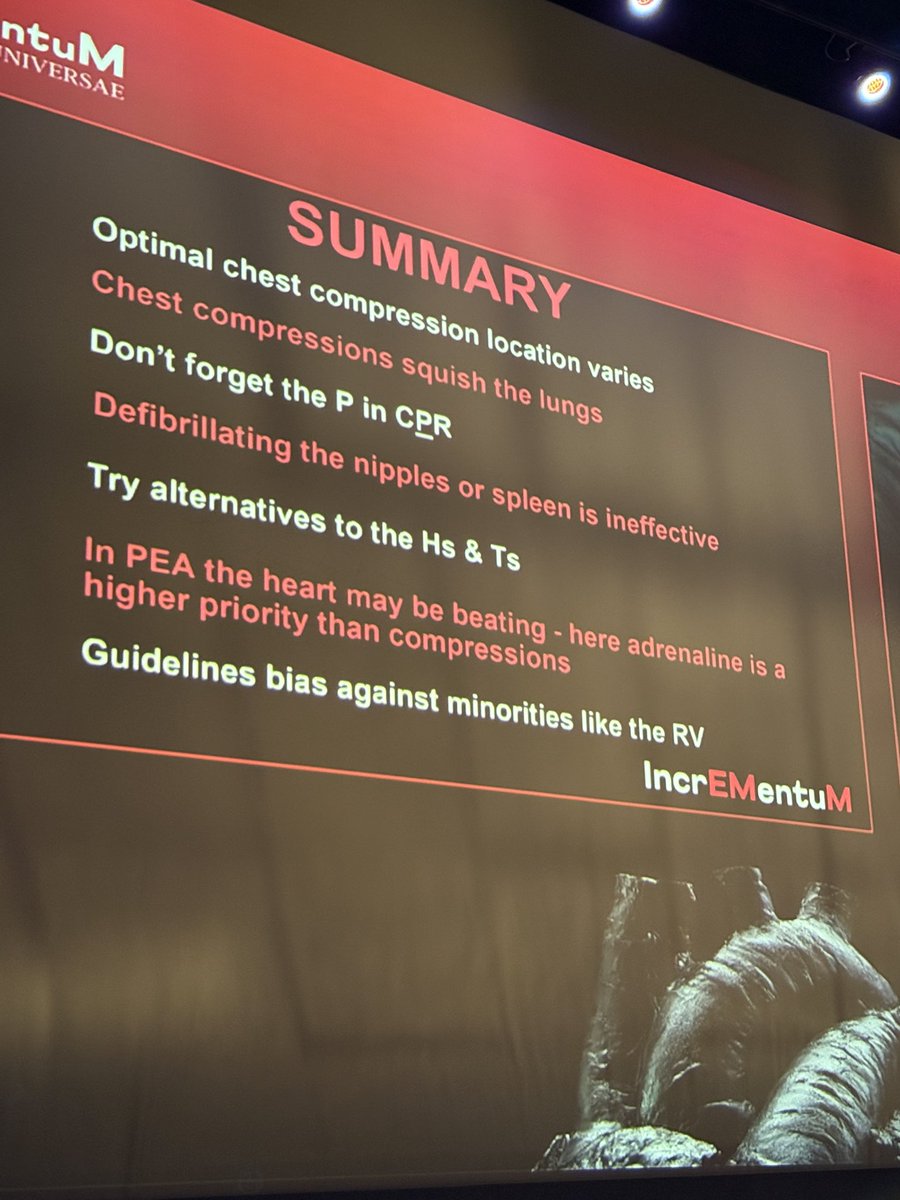
Incorporation of prehospital TOE in cardiac arrest resuscitation is feasible. Identifying the area of maximal compression early in the resuscitation may improve OHCA outcome and aid in the ECPR decision making tree. Larger trials are needed #resuscitation#OHCA#ECPR#prehospital
I underwent explainaesthesia this week and emerged knowing a LOT more about hyperangulated videolaryngoscopy thanks to Nicholas Chrimes https://t.co/6xaiJubJnM
The Netherlands now has nationwide availability of prehospital ECPR! From today, our #HEMS team of Amsterdam is equipped with #ECMO as part of the OnScene trial. Now all Dutch HEMS can provide ECPR. 🚁🇳🇱 More info on https://t.co/I2CmCR1hTb And check out https://t.co/LdcKIoEPKR
(5/x) Finally, here's a case where the ECG heart rate that is displayed LIES!
In this case, you can see that the patient has a bigeminy. The ECG is showing a heart rate of 91, however, there is only ONE arterial line beat for every two electrical beats. Thus, the effective heart rate is actually ~45 BPM.
This is surprisingly common, and without arterial line can be missed. Another clue can be looking at the pulse ox pleth tracing.
This also happens with rapid atrial fibrillation where the HR is reading 130s but only 70-80BPM if you look at the arterial line. That is another indication to me that potentially rate/rhythm controlling the patient will help their hemodynamics.