Great few days at #AUA2026. Grateful to have presented 2 posters, reconnect with my former basic science mentor from Cornell, spend time with my co-resident family, and catch up with old Mexican friends in urology. These are the moments that make the long road feel worth it.
The whole crew showed up to support Department Chair @ctleeuro at #AUA26 as she discussed her work on “Virtual Training to Mitigate Implicit Bias in the Certification of US Urologists: A Feasibility Study from the @ABUrology”👏👏👏
@OSUWexMed@AmerUrological
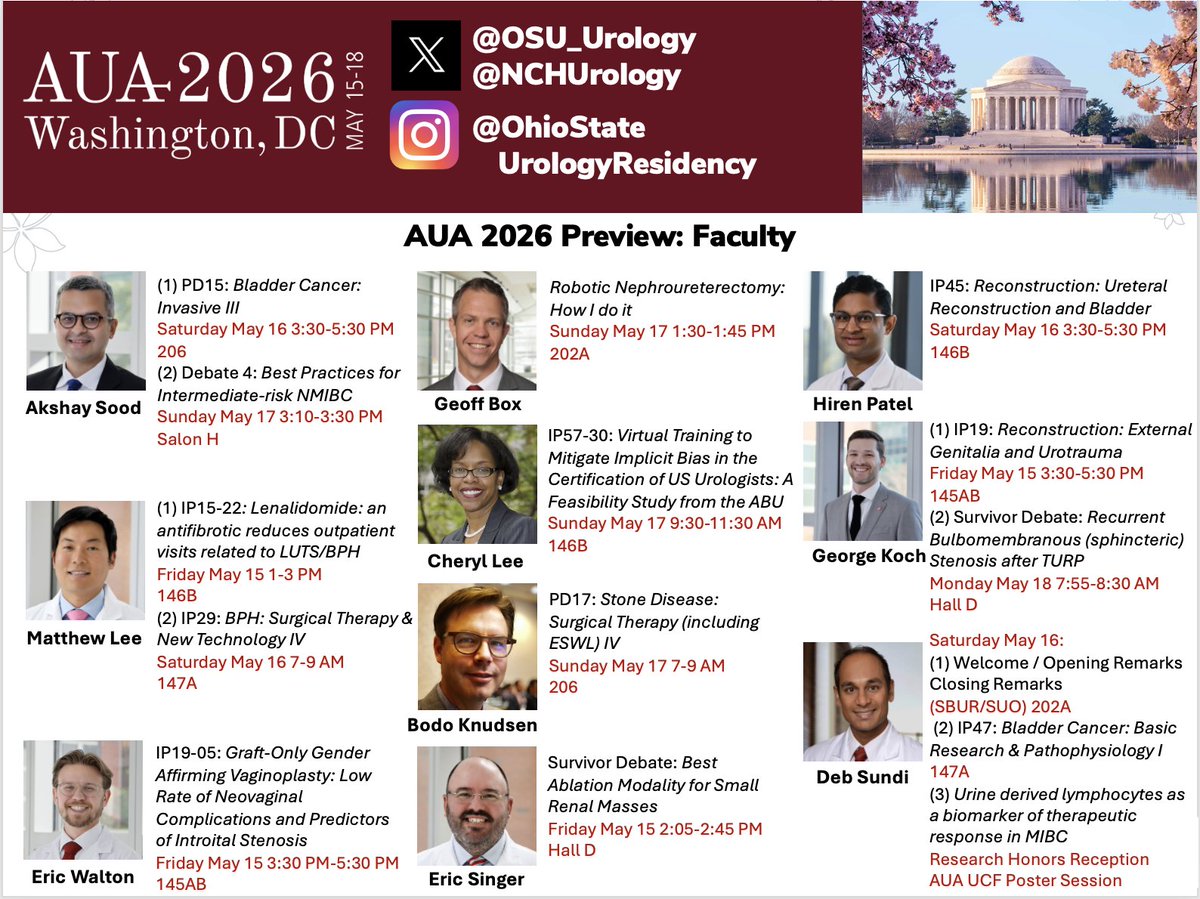
The expertise of Ohio Urology will be on display at #AUA2026 next week!
Our faculty are leading the conversation in urologic surgery, education, innovation, and research through invited talks, podiums, panels, and scientific sessions throughout the meeting.
#AUA26#AUAPreview
Ohio State medical students and research fellows will be presenting their research and scholarly work at this year’s meeting in DC, highlighting the impact of mentorship, curiosity, and collaboration in academic medicine! Congrats! ✨
#AUA2026#AUA26#AUAPreview
Phase 3 KEYNOTE-905/EV-303 trial: Patients with muscle-invasive bladder cancer who are ineligible for cisplatin often proceed directly to surgery. Research evaluating perioperative enfortumab vedotin plus pembrolizumab is summarized in a new Quick Take video. https://t.co/2fDwGvtW3q
Congratulations to Cheryl Lee, MD, who received the Joseph A. Smith Jr. Mentorship Award from the Society of Urologic Oncology (@UroOnc), honoring her impact as a mentor in the fields of urology and urological oncology. ⭐️ https://t.co/AdkbC7BY1g
#OSUWexMed reconstructive urologist Dr. Patel has had a career-long interest in antibiotics and the global threat of antibiotic resistance. He's currently leading a trial on using chlorhexidine lavage to irrigate the urinary tract prior to catheter removal.https://t.co/Wu1NHQ7wAm
IT IS THIS TIME OF THE YEAR AGAIN!
TOP 10 GU clinical trials in 2025!
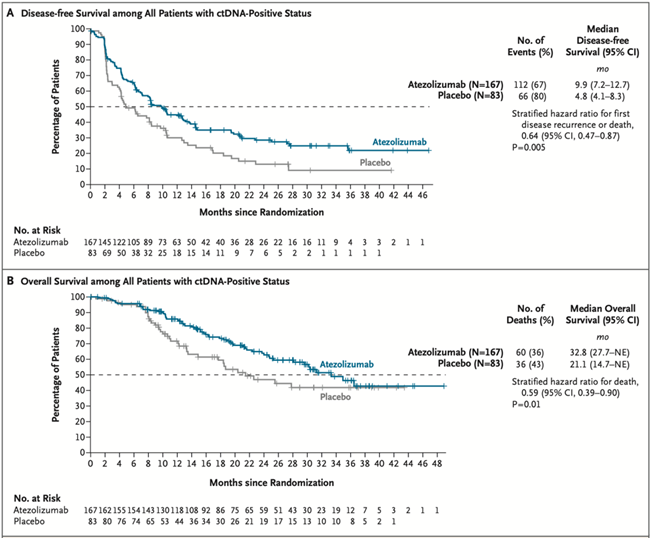
1/ Practice-changing IMvigor011: In ctDNA+ MIBC post-cystectomy, adjuvant atezo improved DFS (HR 0.64) & OS (HR 0.59) vs placebo. ctDNA- pts spared therapy w/ 2-yr DFS ~88%.
@tompowles1@DrYukselUrun@OncoBellmunt@NEJM #ESMO2025 Plenary @myESMO
https://t.co/mbl2VKLZ2N
New paper out ✅
We reviewed 19 studies on Augmented Reality in outpatient care and found consistent benefits in patient understanding, assessment, device interaction, procedural guidance & rehab.
Grateful for the mentorship - more coming soon!
🔗: https://t.co/zlYsH9q56j
Optimal Duration of Androgen Deprivation Therapy With Definitive Radiotherapy for Localized Prostate Cancer: Meta-Analysis
https://t.co/U8xUGsAl2e
Meta-analysis of over 10,000 patients from 13 randomized trials found that the survival benefit of androgen deprivation therapy (ADT) combined with radiotherapy is highly dependent on both treatment duration and patient risk profile, with diminishing returns beyond roughly 9–12 months and increasing non–cancer-related mortality with prolonged therapy. Optimal duration varied by disease severity—shorter or no ADT for lower-risk intermediate disease, longer courses for higher-risk groups—highlighting that extended therapy is not universally beneficial.
Because longer ADT improves cancer-specific outcomes but also increases other-cause mortality, the study emphasizes tailoring duration based on individual risk, comorbidities, life expectancy, and patient preference rather than applying uniform treatment lengths. #ProstateCancer
@NicholasZaorsky@yilun_sun@StatMatt9@DrHowardSandler@drjefstathiou@Soum_Roy_RadOnc@DrPaulNguyen@jeshoag@PBarataMD@angela_jia_@MSteinbergMD@AmarUKishan@DrSpratticus@OncoAlert 🚨
@Silke_Gillessen@AOmlin@weoncologists
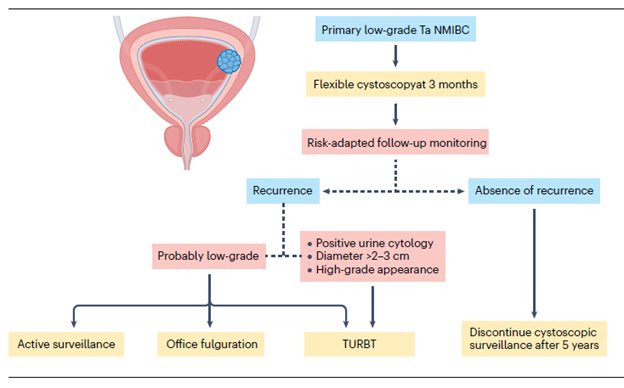
“Low-grade Non–Muscle-Invasive Bladder Cancer: Molecular Landscape, Treatment Strategies, and Emerging Therapies” - just published in Nature Reviews Urology @NatRevUrol. This State-of-the-Art review by Drs. Roger Li @UrogerliMD, Lexi Wen, and colleagues @philippespiess@spsutkaMD@LDyrskjot@DrShariat@UroDocAsh offer an outstanding overview of advances in molecular biology, diagnosis, targeted therapies, and clinical management for #bladdercancer. A great honor to be part of this effort.
Summary:
The management of low-grade non–muscle-invasive bladder cancer (NMIBC) is undergoing rapid evolution, driven by a growing recognition of the need for nuanced, risk-adapted strategies that minimize overtreatment. Yet widespread adoption of de-escalated approaches remains limited by the lack of well-defined, evidence-based guidelines tailored to this favorable-prognosis disease subset. Clear recommendations - particularly regarding surveillance frequency, duration, and criteria for de-intensified care - will likely require international consensus efforts supported by robust prospective data.
A major priority for future research is refining risk stratification. Distinguishing patients at truly increased risk of progression from those with indolent disease will enable more personalized management, including appropriate use of active surveillance and reduced surveillance intensity. Advances in molecular profiling, urine-based biomarkers, and AI-assisted pathology show promise for identifying meaningful biomarkers and histologic patterns to support such stratification, but rigorous prospective validation remains essential before broad clinical adoption.
AI integration into clinical workflows offers additional opportunities to enhance diagnostic accuracy, predict recurrence or progression, and support individualized decision-making. Multimodal models capable of real-time risk assessment may eventually guide therapy selection, but challenges - including the need for diverse training datasets, transparent algorithms, and clear ethical and regulatory frameworks - must be addressed before routine clinical use.
Despite favorable overall outcomes, managing low-grade NMIBC remains challenging owing to high recurrence rates and continued reliance on invasive cystoscopy and imperfect biomarkers. Until emerging diagnostic tools are validated, established clinicopathological systems such as the IBCG risk stratification model will continue to guide treatment decisions. Patients with multiple risk factors generally warrant intravesical therapy, while those without risk factors may be reasonable candidates for active surveillance. The ongoing BCG shortage further underscores the need to balance clinical benefit with treatment burden and to evaluate new intravesical therapies against their potential financial and clinical toxicity.
Meaningful progress in low-grade NMIBC will depend on prospective validation of emerging technologies and therapies, paired with thoughtful integration into evidence-based guidelines. By aligning molecular insights, technological innovation, and risk-adapted clinical practice, the field can improve outcomes while reducing unnecessary interventions and surveillance for this common, yet often overtreated, disease.
The article is available at the following link:
https://t.co/Hkzge1HLDo
BREAKING🚨: The #FDA has approved the combination of pembrolizumab and enfortumab vedotin as neoadjuvant treatment followed by adjuvant treatment after cystectomy for patients with cisplatin-ineligible MIBC. https://t.co/ceKYWsu0Ab
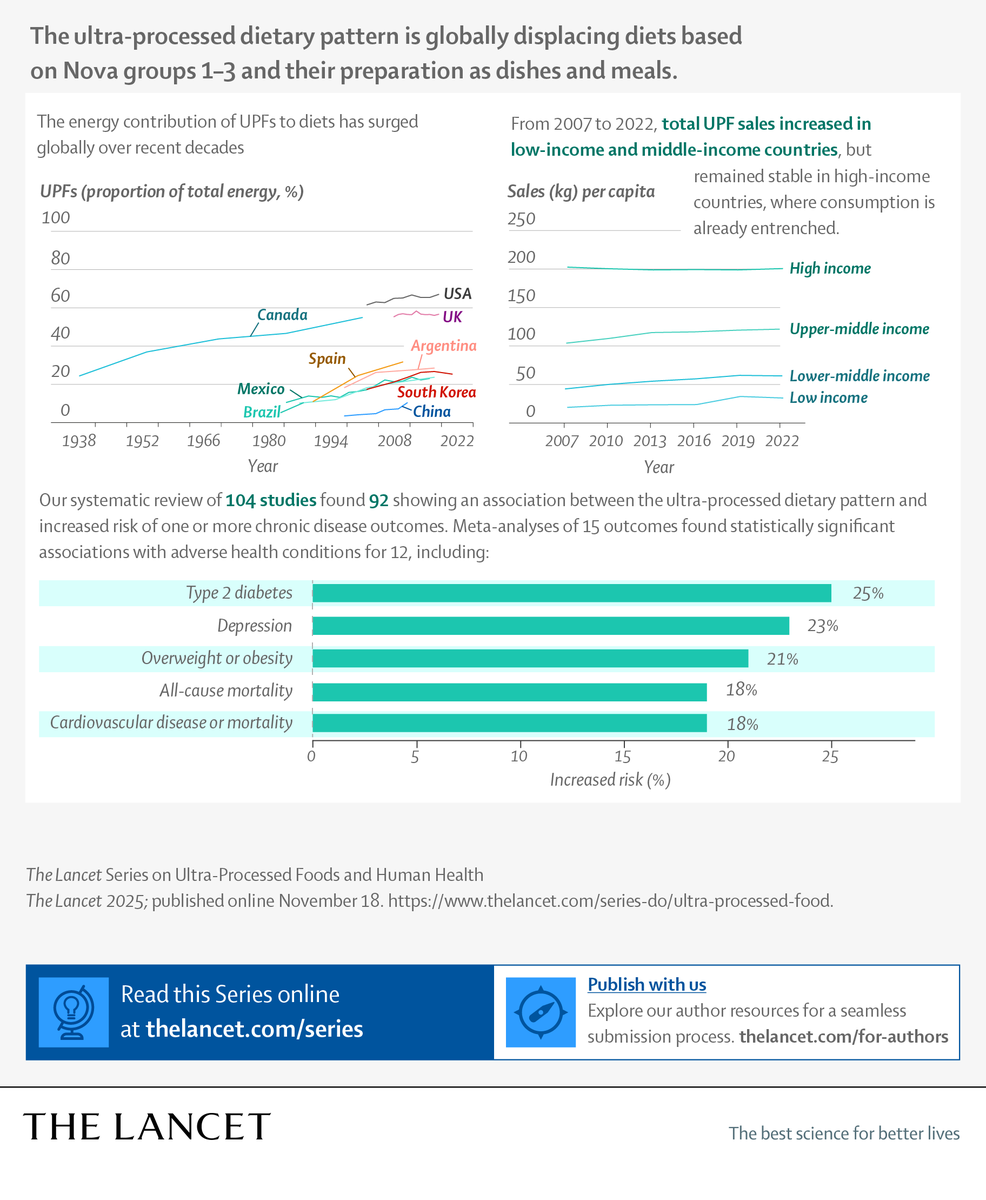
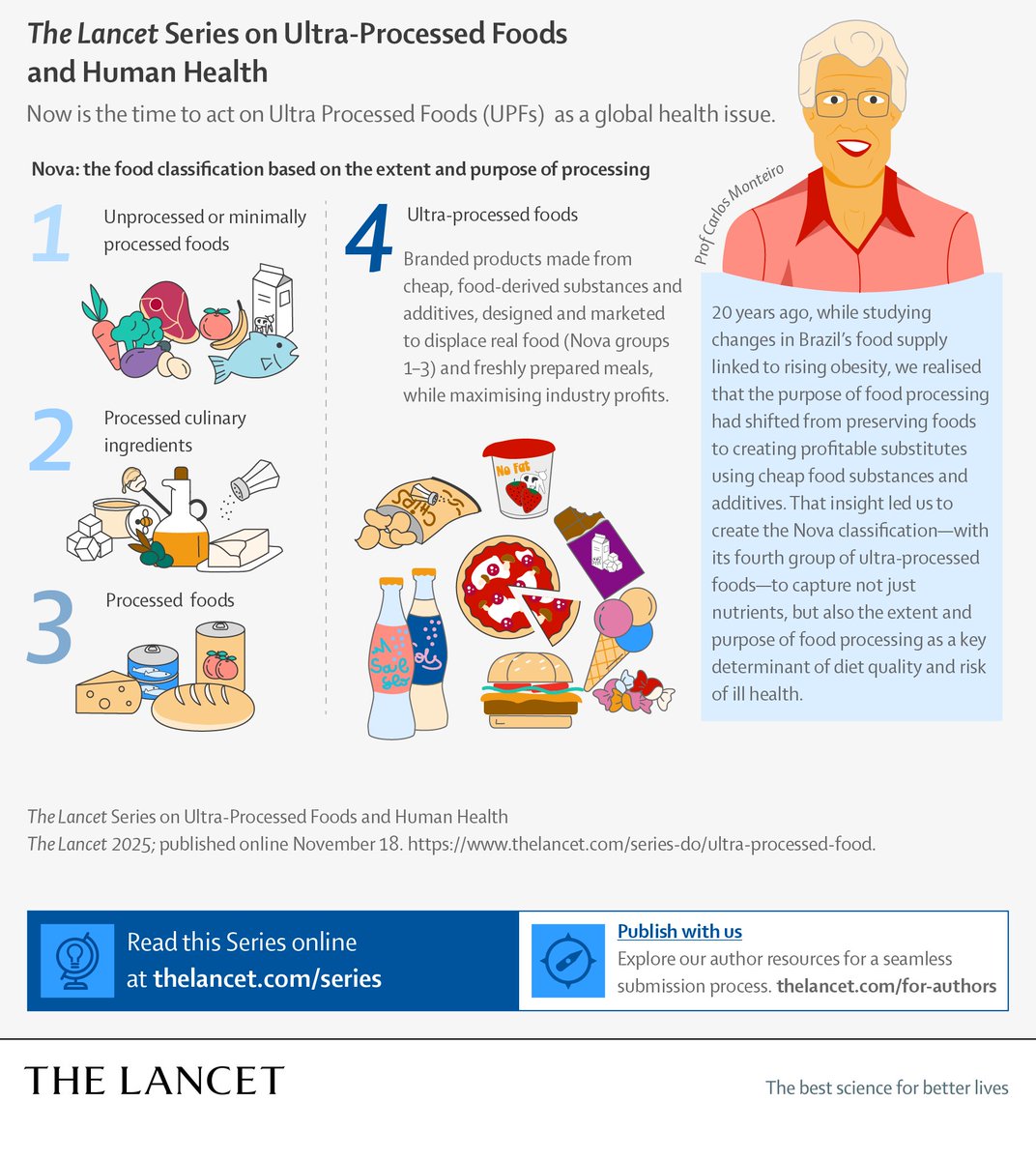
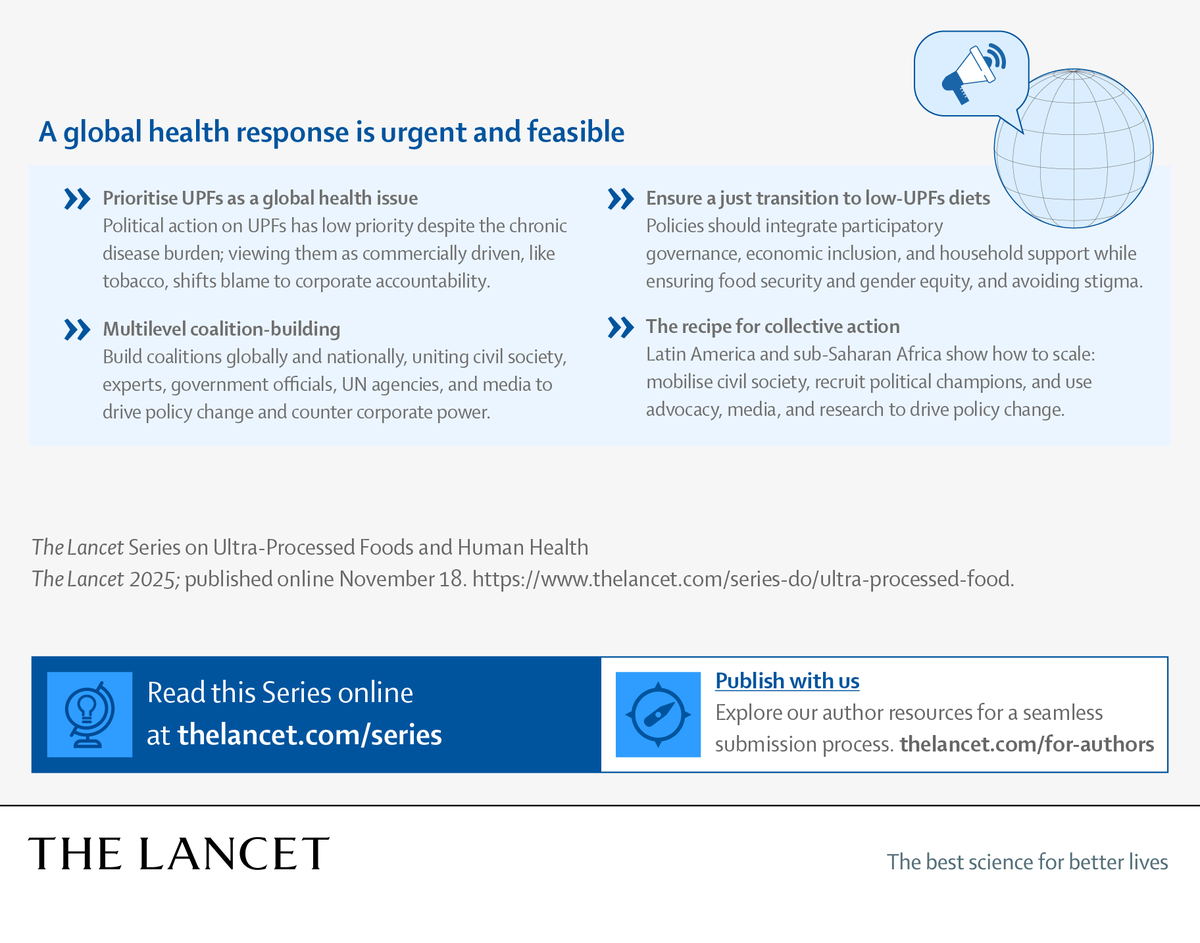
Ultra-processed foods – what’s the impact?
In a new Lancet Series, experts warn a global rise in #UPFs presents a growing public health threat.
Read the evidence & policy recommendations ⬇️
https://t.co/cKavYNYlcQ