I think this was one of the most important datasets for breast oncologists at #ASCO26: the ET-use analysis in the HR+/HER2+ cohort of HER2CLIMB-05.
In HER2CLIMB-05, PFS curves in HR+ patients who received ET appear to be maintained for a longer period, with a lower rate of early progression. In contrast, the curve in patients who did not receive ET starts to decline earlier and more prominently.
This was not an ET-randomized analysis. So it would be methodologically wrong to say directly that “ET improved PFS.” But the direction of the curves is highly consistent with the biology of HR+/HER2+ disease:
Suppressing HER2 while leaving the ER axis untreated may represent undertreatment, particularly in the maintenance setting.
PATINA provides the cleanest comparison here. In PATINA, ET was not the question; it was the backbone. All patients received anti-HER2 therapy plus ET. Even the control arm included ET. Palbociclib was added on top of this backbone and improved PFS from 29.1 to 44.3 months.
So one of the key messages of PATINA was not only “add a CDK4/6 inhibitor.” The more fundamental message was this:
In HR+/HER2+ metastatic breast cancer, the biological backbone of maintenance therapy should be anti-HER2 therapy plus ET.
HER2CLIMB-05 reminds us of the same point from another angle. Disease control appears to be maintained longer in patients receiving ET, while early progression seems more evident in those not receiving ET.
In my view, maintenance treatment in HR+/HER2+ metastatic breast cancer should no longer be thought of simply as “continue anti-HER2 therapy.”
Anti-HER2 therapy is the backbone.
But the ER axis should not be left untreated.
In this patient group, maintenance ET should not be viewed as an optional add-on; omitting it should require a clear clinical justification.
The treatment landscape for HR+/HER2− metastatic breast cancer is evolving rapidly. With biomarker-driven therapies targeting ESR1, PIK3CA, BRCA, and the growing role of next-generation antibody-drug conjugates such as T-DXd, Dato-DXd, and sacituzumab govitecan, patients now have more effective and personalized options than ever before.
#BreastCancer #MBC #oncology #bcsm
#ASCO26
Does CDK4/6i really work in ER-low disease?
I had also really wanted to study the efficacy of CDK4/6 inhibitors in ER-low tumors, but I could not collect enough data. This study addresses exactly this important question. First of all, congratulations to the investigators.
In ER-low HR+/HER2− MBC, CDK4/6i + ET does not seem to deliver the expected HR+ benefit: PFS was 2.9 months. In ER-high patients, PFS was 23.3 months.
Despite the small sample size and the inherent limitations of a retrospective study, the observed behavior is consistent with what we would expect from ER-low tumors. ER-low disease should not simply be placed into the classic HR+ category with automatic CDK4/6i + ET. This subtype behaves closer to TNBC.
Adjuvant T-DXd is approved for pts with HER2+ BC and high-risk RD by DB05 criteria. What about pts with lower risk RD? We looked at ~10.000 pts in Flatiron, finding that 52% have low-risk RD, with 3yr DRFS 94%, suggesting that T-DM1 remains an adequate SoC for them. #ASCO26 Ab545
JUST IN: @FDA approves adjuvant PD-L1 inhibitor Atezolizumab in Muscle-Invasive Bladder Cancer post surgery & ctDNA MRD (+) by @NateraGenetics Signatera CDx approved as companion diagnostic.
MRD-guided adjuvant therapy is moving into practice in Bladder Cancer!
FDA link: https://t.co/DPjLN6Ag2Z
Very important data. Even in the absence of oral SERD at crossover, there is no apparent OS benefit as yet for switch based on molecular ESR1mut detection without radiological progression. And in current practice, all patients would get an oral SERD at radiological/clinical PD
Results from BioItaLEE published in CCR: with a blood draw after 2 weeks of treatment, you can predict whether a patient will remain on 1L letrozole/ribo for a median of 1 vs ~2 yrs. Congrats @BianchiniGP and colleagues for the publication! 🇮🇹💪 https://t.co/gedniOWEMz
🌟 The Abscopal Effect : When local radiation has systemic impact ✨
👥 What is it?
Radiation to a single tumor site → unexpected regression of distant, non-irradiated tumors.
⚙️ How does it work?
• 🔥 Radiation kills cancer cells → releases tumor antigens
• 🛡️ Immune system gets activated → T-cells attack metastases elsewhere
• 💉 Often boosted with immunotherapy (RT + ICI combos)
📊 Reality check
Rare in clinic, but growing evidence with IO combinations.
💡 Takeaway
Radiation = not just local control… it can spark systemic anti-tumor immunity.
👉 Turning the body into its own “vaccine factory.”
#OncoTwitter #RadOnc #medtwitter #ImmunoOncology
@OncoAlert@astro@asco@myesmo
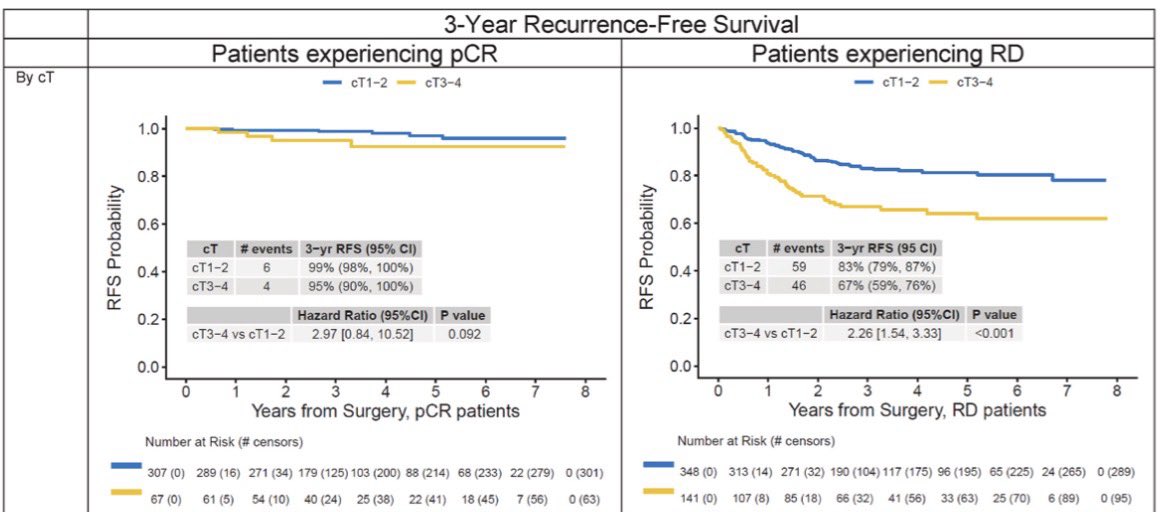
New real-world study in early HER2+ and TNBC after neoadjuvant therapy:
In this study pCR remained the strongest prognostic marker. In 863 patients, 3-year RFS was 98% with pCR vs 79% with residual disease; 3-year OS was 100% vs 88%. In HER2+, 3-year RFS was 99% with pCR vs 87% with RD; in TNBC, 97% vs 72%.
Baseline cT/cN/subtype predicted worse outcomes mainly in patients with residual disease. Among patients achieving pCR, baseline stage was not significantly associated with RFS or OS in this cohort.
In this study pCR appears to largely mitigate the adverse effect of initial tumor burden, but residual disease still identifies a clearly higher-risk population needing escalation/novel strategies.
@CCortiMD@stolaney1@oncodaily
👉 https://t.co/gXjmCHnVjf