We talk a lot about HFrEF. But what about HFpEF and HFmrEF?
@mvaduganathan@gcfmd@SJGreene_md@BiykemB@hfcollaboratory@HFA_President@HSkouri
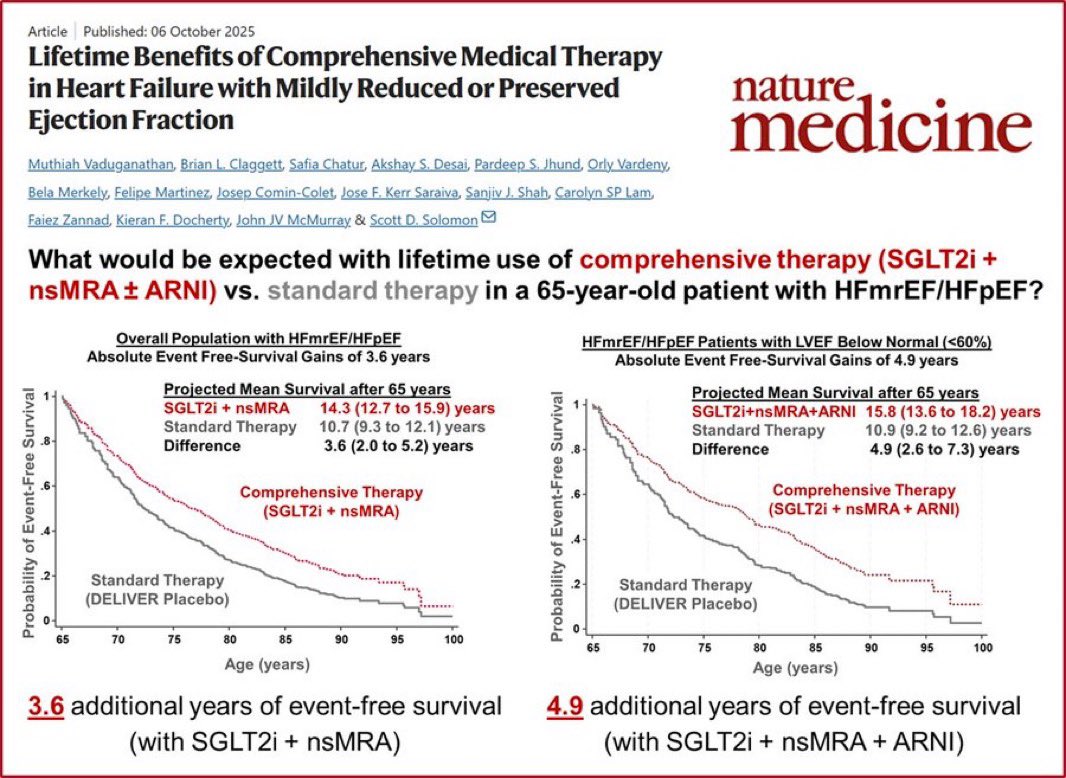
This Nature Medicine study answers the question most patients actually ask: “How much longer will I live?”
For a 65-year-old with HFmrEF/HFpEF:
📌 SGLT2i + nsMRA vs. standard therapy:
→ +3.6 years of event-free survival
📌 SGLT2i + nsMRA + ARNI (LVEF <60%):
→ +4.9 years of event-free survival
Nearly 5 extra years. Not months.
Comprehensive therapy for HFpEF/HFmrEF isn’t optional anymore — it’s the standard.
Vaduganathan et al., Nature Medicine, Oct 2025
#HeartFailure #HFpEF #HFmrEF #SGLT2i #Cardiology #CardioTwitter #MedTwitter
🫀 Cardiomyopathies: the real risk is not the disease… it’s missing it
We often focus on treatment.
But this paper highlights a more uncomfortable truth:
👉 failure to diagnose cardiomyopathies is still a major problem
⚠️ The striking finding
Most medicolegal cases are not about complex management.
👉 They are about:
Missed diagnosis
Delayed recognition
Poor communication
➡️ The basics—not the advanced care—are failing
📊 Even more concerning
Many cases present with cardiac arrest or sudden death (~59%)
Diagnosis often made too late—or never
👉 The first presentation = the last opportunity
🧠 Where are we missing it?
Primary care → no ECG / delayed referral
Specialist level → misinterpretation or under-recognition
Pathology → misclassification (e.g. CAD instead of cardiomyopathy)
➡️ Failure happens across the entire pathway
🧬 The hidden consequence
👉 This is not just about one patient
Cardiomyopathies are often genetic
➡️ Missed diagnosis =
No family screening
Preventable deaths in relatives
⚠️ Arrhythmogenic cardiomyopathy (ACM)
Interestingly:
👉 Rarely reported in litigation
Not because it’s rare—
👉 but because it’s hard to diagnose
💬 And then comes communication
One of the most frequent failures:
👉 Not informing families
➡️ The medico-legal implications are huge
➡️ The clinical implications are even bigger
🤖 A new layer of complexity: AI
Increasing use in ECG/imaging
But who is responsible for interpretation?
👉 We are entering a new era of shared (and unclear) liability
🌍 System-level issue
Need for specialist inherited cardiac centres
Better education
Structured diagnostic pathways
➡️ Diagnosis is not just clinical skill
👉 it’s system design
🔥 Take-home
Cardiomyopathies are not rare.
They are underdiagnosed.
👉 And in this field:
Missing the diagnosis is the biggest risk factor of all
#Cardiology #Cardiomyopathy #SCD #Genetics #CardioGenetics #MedicalEducation #PrecisionMedicine 🫀🧬
https://t.co/nQUS82H3Om
🚨 Can echocardiography really exclude HFpEF? New data say: not reliably.
A large, invasive hemodynamics–validated study tested the updated 2025 ASE diastolic function grading algorithm in patients with confirmed HFpEF — and the results are eye-opening. 👀
🔍 Key finding:
Among ambulatory patients with invasively proven HFpEF, ~68% were classified as “normal” or Grade 1 diastolic dysfunction by the new ASE criteria. Yet >60% of these patients already had elevated filling pressures at rest, and many worsened dramatically with exercise.
🏃♂️ Stress echo underperformed:
In patients labeled Grade 1 (where exercise testing is recommended), the ASE 2025 stress criteria detected HFpEF in only ~10% — a false-negative rate >90%. Even under “best-case” assumptions, sensitivity remained poor.
🏥 Volume status matters:
Diastolic grades shifted substantially between decompensated and recompensated states. After diuresis, over 50% of hospitalized HFpEF patients reverted to normal or Grade 1, highlighting how load-dependent and unstable diastolic grading can be.
📉 Diagnostic performance:
Overall discrimination for HFpEF vs non-cardiac dyspnea was modest (AUC ~0.61) — inferior to probability-based tools like H₂FPEF, especially when combined with functional testing.
⚠️ Prognostic paradox:
Patients with HFpEF labeled “normal” or Grade 1 still had a ~5-fold higher risk of death or HF hospitalization compared with controls.
💡 Bottom line:
🛑 Normal diastolic function ≠ no HFpEF.
Echocardiography remains essential — but diastolic grades must be interpreted within pretest probability frameworks, not used in isolation to rule out disease.
#EHJCVI 📢 New #EACVI Consensus Statement🚨 Role of multimodality imaging in the management of #HCM in 2025🫀In-depth, state-of-the-art document focusing on the role and advances of #CVImaging techniques in #HCM💡#echofirst#WhyCMR#CVNuclear#CCTV ⏩ https://t.co/JbPOo7bmz0
5/
I was delighted to see so many national societies contributing to joint sessions, alongside our sister societies from across the world—a powerful demonstration of collaboration and unity.
Amazing second day with insightful talks and tutorials. So happy to be here, having the opportunity to present and share experiences with professionals! #EACVI2025
A fantastic start to #EACVI2025 with the wonderful presentation of Prof. @leylaelifsade — it is always truly inspiring to meet and listen to you. Grateful for sharing your expertise and guidance!
Multimodality imaging in advanced heart failure. A clinical consensus statement of the #HFA of the ESC. Part 1: Multimodality imaging for the evaluation of patients with advanced HF
https://t.co/6U8Miqjtvl
@ESC_Journals@HanCardiomd@AmrAbdin10@GiuseppeGalati_
A fresh publication for a perfect weekend read! 📚✨
Clearly summarized and practical:
Right heart catheterization in heart failure – indications, interpretation, and pitfalls 🫀📊
https://t.co/UfK8f8Ikbp
It was a great pleasure to present in front of leading experts and colleagues from around the world!
So much to learn from their expertise, grateful for the opporturnity!
#HeartFailure2025
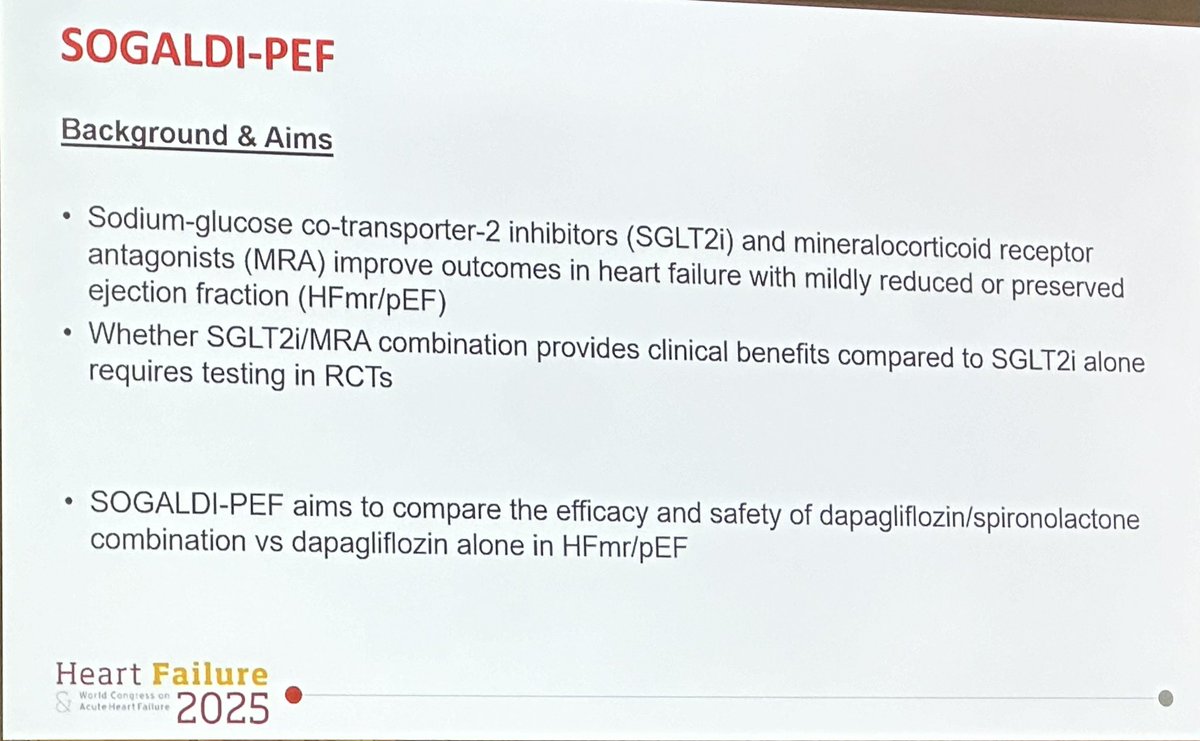
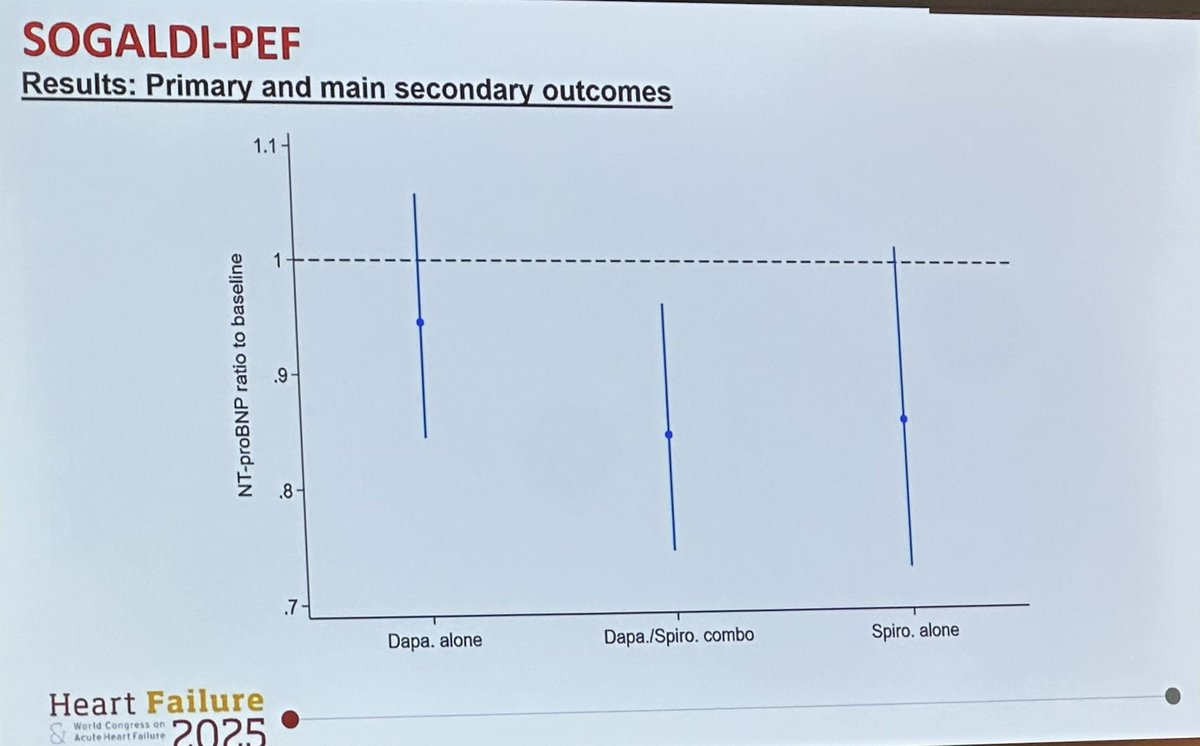
📢 In HFmr/pEF patients, combination therapy with SGLT2 inhibitors and MRAs leads to a greater reduction in NT-proBNP compared to either agent alone✅
However, it is associated with a more pronounced decline in eGFR❗️
Balancing benefits and risks is key!
#HeartFailure2025
📢Excited to announce that our study on the new prognostic score, ‘CALLY Index’, in acute coronary syndrome is now published in Biomarkers in Medicine! Huge thanks to our amazing team!
Full article: https://t.co/4NGsqITAER
Excited to share that our case has been selected for the HFA Congress 2025!
Can’t wait to connect with experts, share knowledge, and learn about the latest advancements! #HeartFailure2025
It’s always a pleasure to meet and learn from your experience! Thank you for this amazing presentation, your valuable time, and your kind guidance! @esrakaya_dr