🫀#HeartFailure26 comes to a close after an incredible few days of science, collaboration, & innovation.
In this special message, HFA President Prof. @MarcoMetra reflects on: - The truly global HF community gathered from all over the world - The outstanding quality of science & abstracts presented - Exciting new initiatives including #HFAUnplugged - and The continued growth of the Heart Failure Association community worldwide
Thank you to everyone who made #HeartFailure26 such a remarkable congress👏
#HFA_ESC @escardio #HFAmotions
🫀 What happens when long-term low-dose #digoxin is suddenly withdrawn?
Blinded withdrawal analysis from the #DECISION trial presented at #HeartFailure26 by Prof. Peter van der Meer:
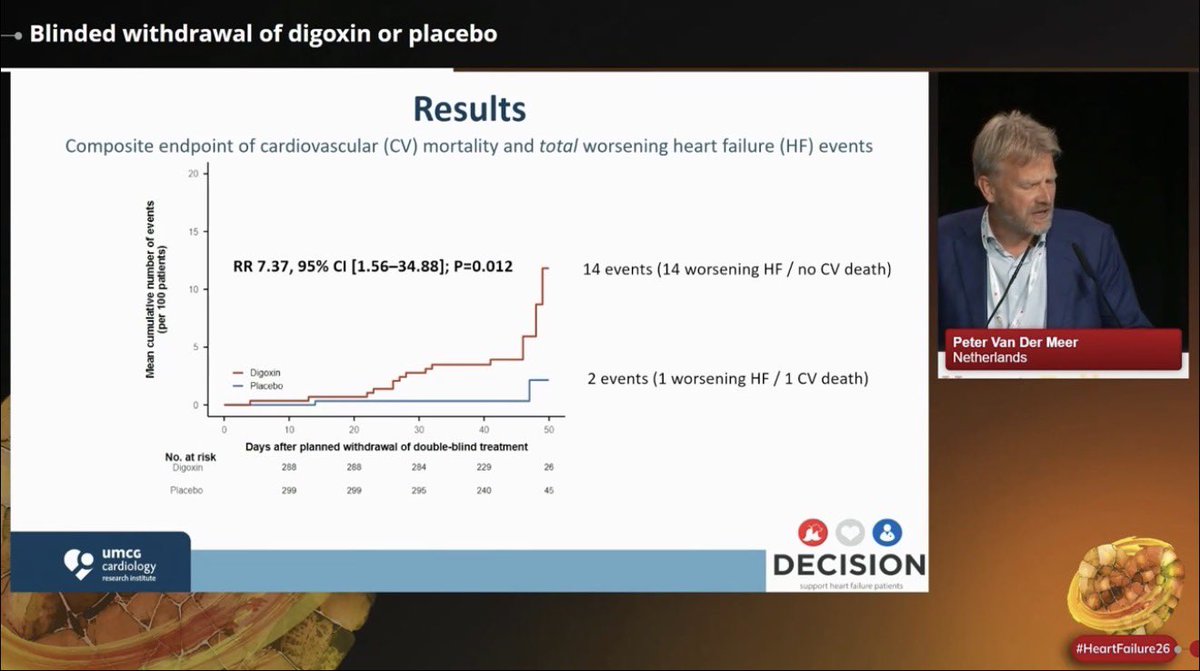
📍Digoxin withdrawal was associated with a ~7x increase in worsening HF events over just 6 weeks
📍14 worsening HF events occurred after digoxin withdrawal vs only 2 events in placebo withdrawal
📍Withdrawal was accompanied by: ⬆️HR,⬇️ SBP, ⬆️NT-proBNP, ⬇️eGFR
📍⚠️caution when stopping long-term low-dose digoxin in pts with HF & LVEF <=50%
@escardio@HFA_President@jozinetm
What I learned the hard way in #HeartFailure care?
Not every setback means failure.
Sometimes the missed opportunity, rejected papers, difficult case, or moment of being overlooked becomes the experience that sharpens your clinical judgment, resilience, & purpose.
In our career, growth often comes quietly:
🫀listening more carefully
🫀staying curious
🫀learning from patients & your mentors
🫀building consistency
🫀showing up again
Early-career setbacks can become the foundation for future impact, if we keep going🥹❤️
Fantastic panels & sharing @KlausKWitte@ARakisheva@noshreza@corneliacrm & Floran Sahiti #HFAyoung
@escardio@HFA_President@jozinetm@MarcoMetra
🫀Could RAAS inhibition improve hemocompatibility outcomes in patients supported with durable #LVAD therapy?
Presented by @ameeshisath at #HeartFailure26:
📍Sustained RAAS inhibitor exposure over 2 years was associated with a 33%⬇️ in hemocompatibility-related adverse events
📍Non-surgical bleeding, particularly GI bleeding, was significantly ⬇️ with RAAS inhibition
📍Outcomes appeared independent of MAP, INR, or aspirin use
📍Combination #RAAS blockade including #MRAs on top of ACE/ARB/ARNI showed greater effectiveness than single-agent RAAS inhibition alone
📍Findings were directionally consistent across both HeartMate 3 & HeartMate II, suggesting a class-level effect rather than device-specific benefit
📍These data support neurohormonal modulation as a complementary strategy alongside LVAD technology to optimize long-term outcomes
@escardio@HFA_President #MCS #GDMTworks
💊 Practical algorithm for diuretic resistance in acute HF from #HeartFailure26— this is the slide to save!
Start: Furosemide 120-160 mg
↓ Still congested?
Add Chlortalidone 12.5-50 mg/24h
↓ Still congested?
Tailor to the problem:
• Metabolic alkalosis → Acetazolamide 120-500 mg/24h
• Hyponatremia → Tolvaptan 15-50 mg/24h
• rLVEF + hypopotassemia → MRA 25-100 mg/24h
And running through the whole algorithm:
➕ Add iSGLT2 throughout
➕ Add sacubitril/valsartan if LVEF <49%
➕ Consider parenteral route if oral absorption is the issue
Clean. Practical. Evidence-based. 💯
(Adapted from de la Espriella R et al. Nefrologia 2021)
#CardioTwitter #HeartFailure #Cardiology #Diuretics #HFrEF
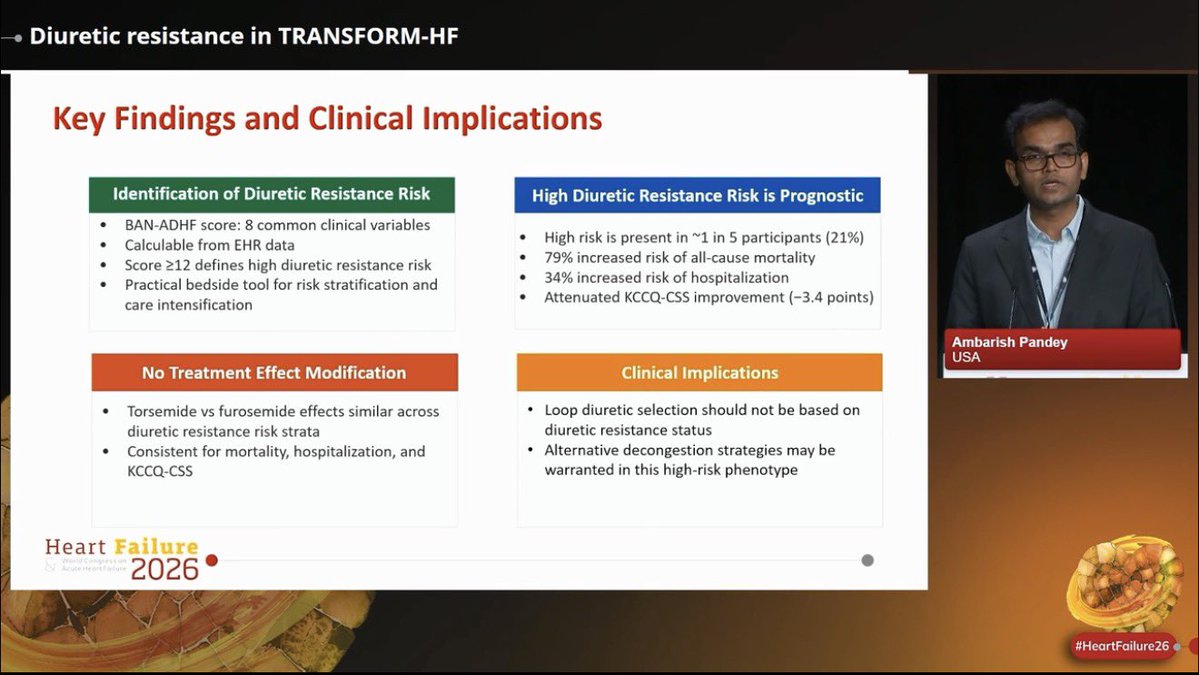
🫀Diuretic resistance identifies a particularly high-risk HF phenotype.
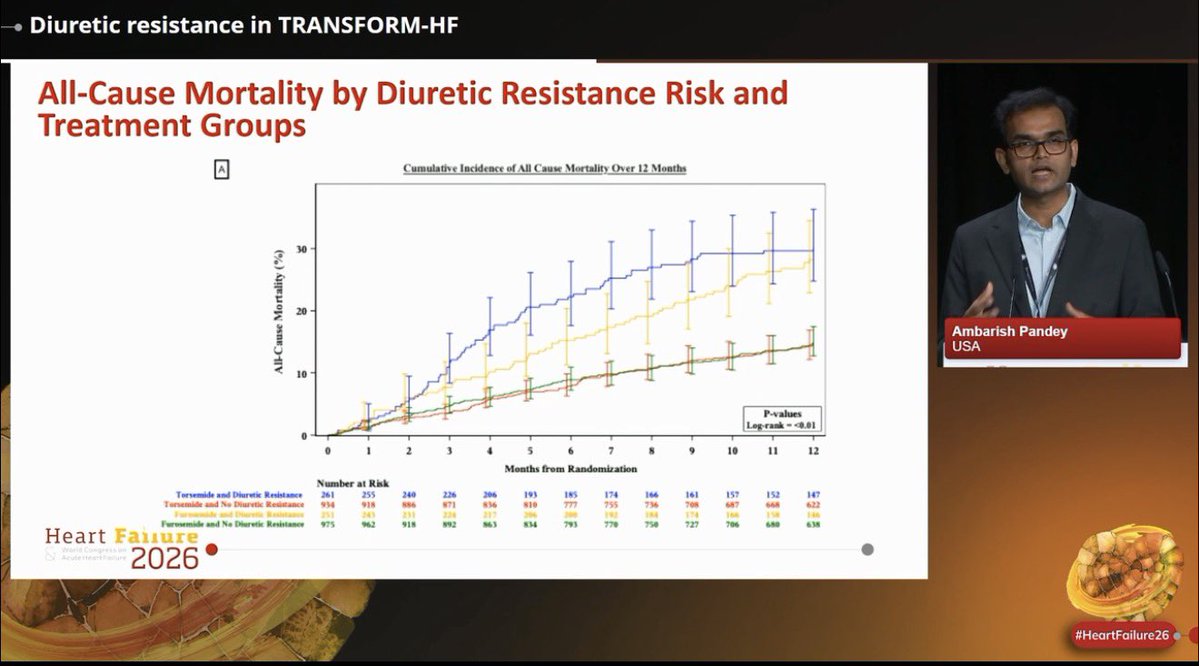
Insights from a post hoc analysis of TRANSFORM-HF presented by @ambarish4786 at #HeartFailure26:
📍~1 in 5 hospitalized HF patients were classified as high risk for diuretic resistance
📍High diuretic resistance risk was associated with:
- 79% higher all-cause mortality
- 34% higher hospitalization risk
- Less improvement in KCCQ-CSS
📍Torsemide vs Furosemide effects similar across diuretic resistance risk strata
📍Loop diuretic selection alone may not overcome the adverse prognosis associated with diuretic resistance
@escardio@HFA_President #DiuresisJedi
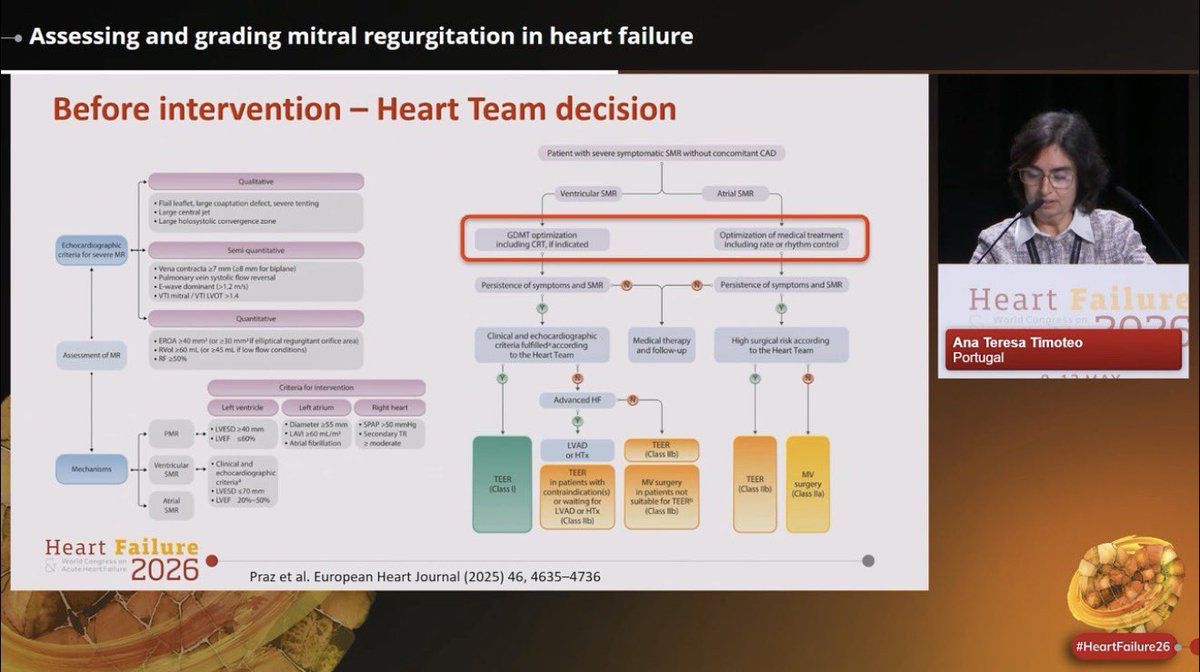
🫀#MR in #HF is far more than “mild, moderate, severe”.
⚠️Accurate MR assessment directly influences HF management & outcomes.
Excellent overview by @anatimoteo46040 at #HeartFailure26 on how we should assess secondary MR in HF:
📍Mechanism matters: Ventricular vs atrial MR, differentiate early
📍MR grading must be multiparametric,
Never rely on a single number alone.
📍Secondary MR is dynamic,
Severity may change after: GDMT optimization, CRT, rhythm/rate control, decongestion. ⚠️Reassess before intervention decisions.
📍Multimodality imaging matters, each provide complementary information on anatomy, mechanism, ventricular remodeling, procedural suitability
📍Heart Team discussion is essential.
📍Quantitative parameters matter most when deciding advanced therapies
@escardio@EACVIPresident@VictoriaDe32503 #EchoFirst #whyCMR #YesCCT #3DEcho #HeartFailure
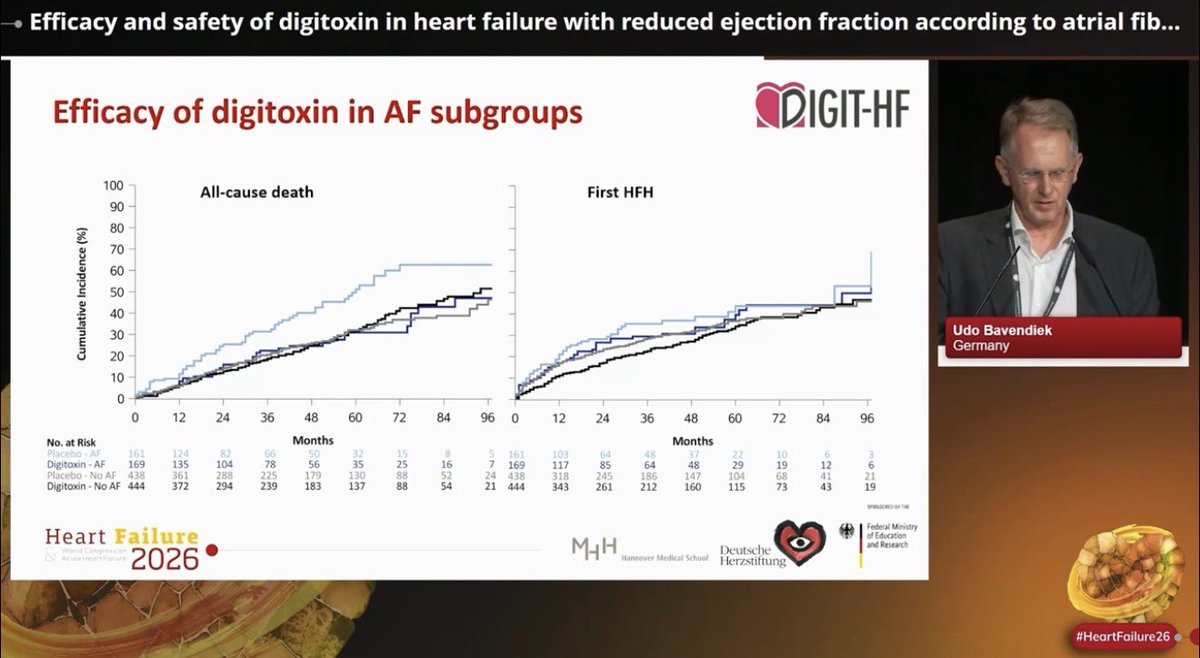
🫀DIGIT-HF subgroup analysis presented at #HeartFailure26 by Prof. Udo Bavendiek, explored the efficacy & safety of #digitoxin in #HFrEF according to #AFib status:
📍HFrEF➕AF represented a clinically higher-risk phenotype with more comorbidities & symptoms
📍Digitoxin ⬇️ the composite of all-cause death or first HF hospitalization irrespective of AF status
📍In AF subgroups: ARR 10.5%, NNT 10 for the primary endpoints
📍The apparent benefit seemed more pronounced in patients with AF, mainly driven by reductions in all-cause mortality
@escardio@HFA_President@MarcoMetra@JBauersachsMD
#HeartFailure26 starts TODAY in Barcelona 🇪🇸🫀
🔥One of today’s highlights:
Hottest Trials (1):
🗓️ 9 May | ⏰ 13:15–14:15 |📍Room 3
🔹SUBCUT HF II: Subcutaneous furosemide to support earlier discharge in acute HF
🔹REDOX-AHF: Restrictive vs liberal oxygen targets in acute HF
🔹Re-PHIRE: AZD3427 in HF with pulmonary hypertension group 2
🔹PRAISE-MR: ARNI in HFpEF with secondary MR
🔹CONDUCT-AF: Randomized multicentre AF study
@escardio@MarcoMetra@jozinetm@WilfriedMullens@GianluSava
The Heart Failure 2026 Congress kicks off in Barcelona this Saturday, May 9. 🔥 Hot Trials Can't Miss on Day 1:UF-CARE;TIM-HF3;SUBCUT HF II;REDOX-AHF & many more…
Stay tuned! #Heartfailure2026#ESCCongress
Registration: https://t.co/WiZfbW8wVm
Platform: https://t.co/x3YmyJ6e5g
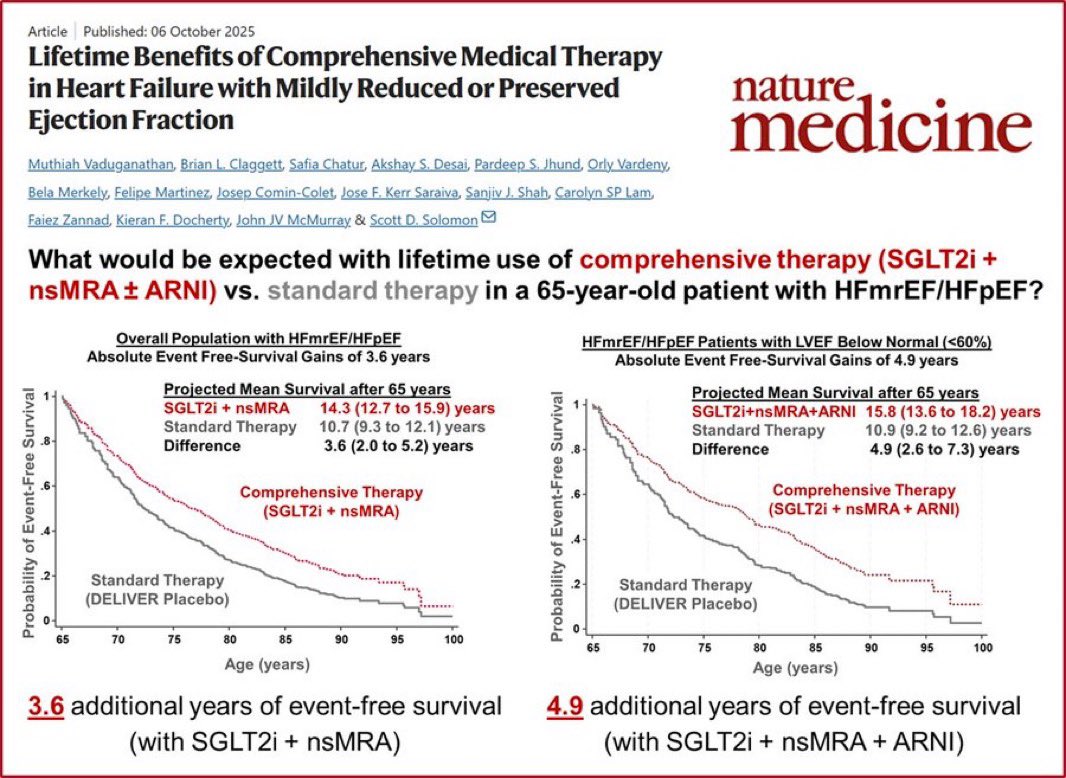
We talk a lot about HFrEF. But what about HFpEF and HFmrEF?
@mvaduganathan@gcfmd@SJGreene_md@BiykemB@hfcollaboratory@HFA_President@HSkouri
This Nature Medicine study answers the question most patients actually ask: “How much longer will I live?”
For a 65-year-old with HFmrEF/HFpEF:
📌 SGLT2i + nsMRA vs. standard therapy:
→ +3.6 years of event-free survival
📌 SGLT2i + nsMRA + ARNI (LVEF <60%):
→ +4.9 years of event-free survival
Nearly 5 extra years. Not months.
Comprehensive therapy for HFpEF/HFmrEF isn’t optional anymore — it’s the standard.
Vaduganathan et al., Nature Medicine, Oct 2025
#HeartFailure #HFpEF #HFmrEF #SGLT2i #Cardiology #CardioTwitter #MedTwitter