CV mortality gaps between Black & White Americans remain among the widest in the US. 2024 📊 shows ⬆️excess deaths+YPLL, persistent disparities across major #CVD categories & partial post‑pandemic recovery
The gap remains unacceptable! https://t.co/y9jwBZoBb1
#JACC#Juneteenth
A missed anticoagulant refill becomes a stroke. A survivable MI becomes financial ruin
In @CircAHA, @prihatha & @DarshaliVyas describe how Medicaid cuts under H.R. 1 don't just ⬇️ coverage, but also create new clinical instability for millions at cardiovascular risk
https://t.co/aaKRVb1SxJ
Celebrating our Inaugural Forum on Feb 21, 2026 at UCSF
Grateful to everyone building something bigger than ourselves. NAPA was created to advocate, uplift & serve. Thanks @DrPanMD, @NCAPIPComms, Dr. Duong, APAMSA UCSF & NAPA Board
Stay connected ➡️ https://t.co/bWJWPGBosy
JACC Stats 2026 is out.
A clear look at U.S. cardiovascular health shows stalled progress, rising burden, and persistent gaps across hypertension, diabetes, obesity, heart failure, and more.
We cannot improve what we do not measure.
@JACCJournals
https://t.co/AHkjsn7cSa
Our new @JACCJournals Cardiovascular Statistics annual report provides a clear-eyed understanding of cardiovascular health in the United States.
Where we stand. Where we've made gains. And where we're falling behind. #JACCStats
https://t.co/ghr90uvqjA
Learning points:
1) #Lupus occurs in 0.1-0.2% of patients taking anti-TNF inhibitors
2) #Rash is the most common manifestation
3) Anti-dsNA is commonly positive (~70%), unlike in drug-induced lupus from non-TNFi agents (<5%)
"It's never lupus" - House, MD
In @JAMA_current, we describe an underrecognized complication from an increasingly prescribed class of biologics for autoimmune disease.
A patient receiving adalimumab for rheumatoid arthritis had ulcerated plaques on the anterior and lateral aspects of the neck, upper chest, and nape and erythroderma on the dorsum of the hands.
What is the diagnosis, and what would you do next? https://t.co/xpr5eM1Kdh
Gemini 3.0 Pro - CORRECT diagnosis and treatment
Grok 4.1 - WRONG diagnosis and treatment
GPT 5.2 Instant - WRONG diagnosis, partially correct Tx
GPT 5.2 Thinking - WRONG
GPT 5.2 Pro - CORRECT dx and tx
Claude Opus 4.5 - CORRECT dx and Tx
OpenEvidence - WRONG (entire differential diagnosis of 9 items did not include the correct diagnosis)
The most advanced models reign supreme.
OpenEvidence missed the mark - as it often does for diagnostic queries. Great for simple evidence-based questions.
MedicalAI Medical AI
What if saving a pneumonia patient was as simple as adding one cheap pill?
A new NEJM RCT from Kenya just showed exactly that. 👇
2,180 adults with community-acquired pneumonia were randomized within 48 hrs to:
🅰️ Standard Care (WHO regimen)
β-lactam (penicillin/cephalosporin) + macrolide (erythro/azithro)
🅱️ Standard Care + 10 days of low-dose steroids
Dexamethasone 6 mg or
Hydrocortisone 160 mg or
Methylpred 30 mg or
Prednisolone 50 mg or
Prednisone 50 mg (bioequivalent dosages)
30-day mortality:
22.6% with steroids vs 26.0% with standard care
➡️ HR 0.84 (95% CI 0.73–0.97), P = 0.02
Adverse events similar. Steroid-related serious AEs: 0.5%.
💡 One low-dose steroid… in hospitals with almost no ICU support… saved lives.
Global pneumonia care may never be the same.
#NEJM #Pneumonia #RCT #GlobalHealth #MedTwitter #EvidenceBasedMedicine #InternalMedicine #CriticalCare #IDTwitter @DrAkhilX @IhabFathiSulima@CelestinoGutirr@Urchilla01@drkeithsiau
Amazing collaboration with my friend @ChingHsuan16@TuftsCEVR, STRONG-HF trialists, and star mentors @AferditaMD & @AnkurFactorial!
We must overcome the urge to go slow and invest in GDMT titration programs to safely & cost-effectively bend the heart failure mortality curve.
What if we could prevent #heartfailure deaths?
What if #therapies already exist?
What if the #cost was worth it?
In @JCardFail, we show the #costeffective promise of rapid GDMT titration from #STRONGHF
Quad therapy $47,000/QALY, Less for the Brits!
https://t.co/Q9QTnff0ic
Evolocumab in Patients without a Previous Myocardial Infarction or Stroke: @NEJM@AHAScience#AHA25
🥸VESALIUS-CV - subtilisin–kexin type 9 (PCSK9) inhibitor evolocumab
😱Summary
👇👇👇
Get this: Coffee suppressed atrial fibrillation!
Unexpected results for recurrence from a randomized trial in participants after cardioversion from AF
#AHA25@JAMA_current ☕️ https://t.co/70dPI2R84C
New @JACCJournals Editor’s Page: A Disquieting Plateau
🫀 Cardiovascular mortality progress has stalled
📉 In some areas, it’s reversing
💡 We must confront what’s happening on our watch—and what comes next
👉 https://t.co/60dIQAMI7T
#CardioTwitter#HealthEquity@JACCJournals
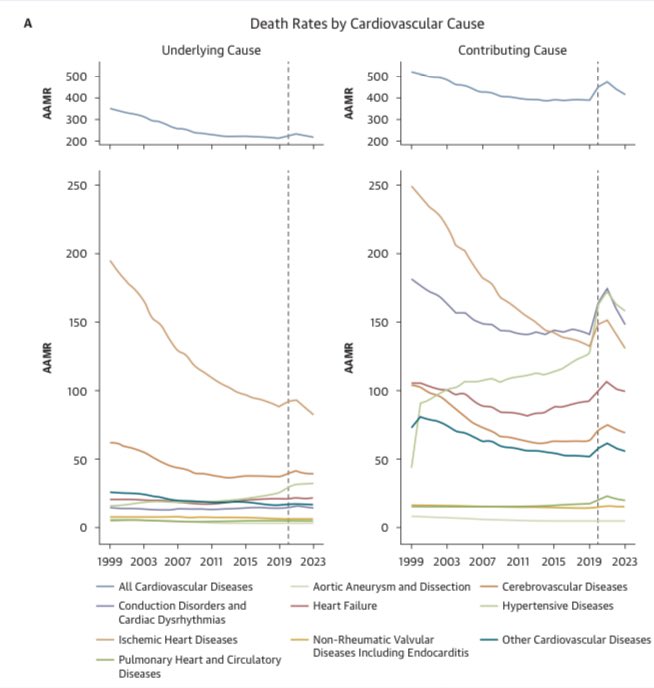
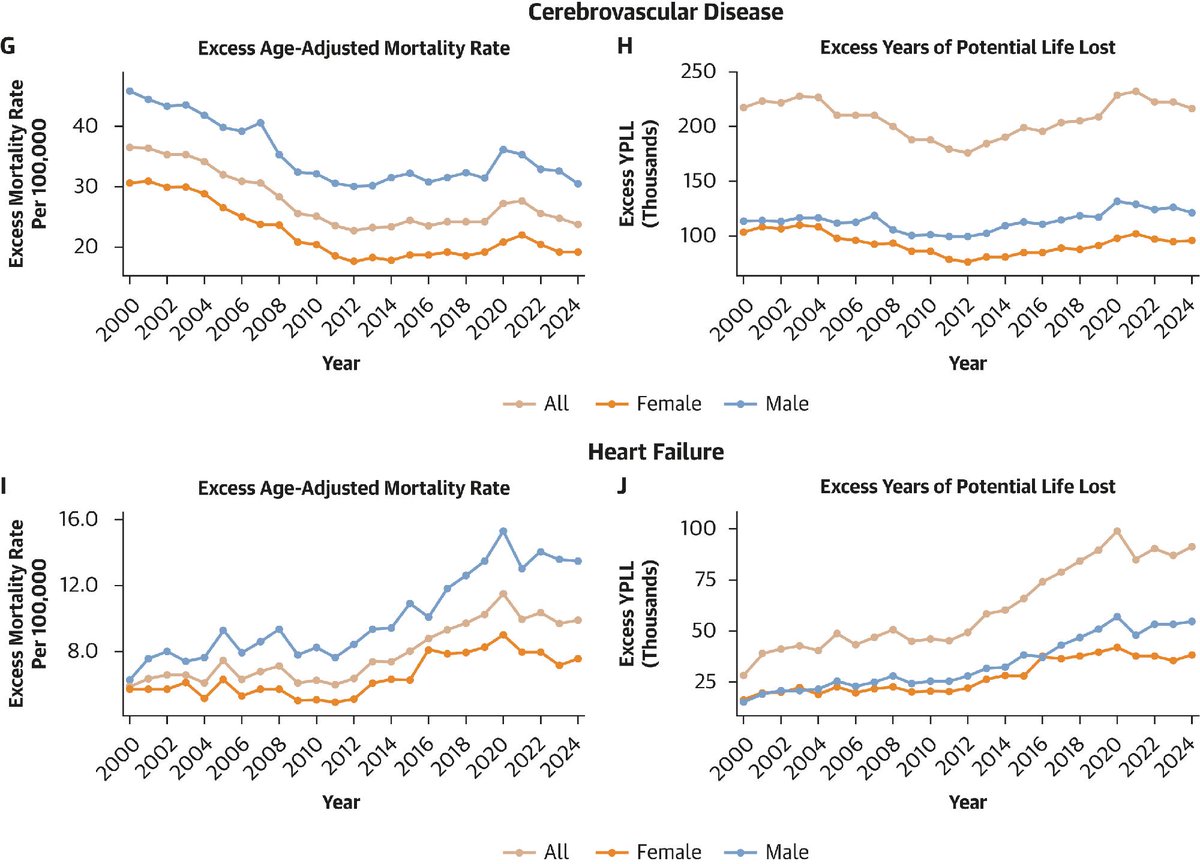
The timing of the observed plateau in cardiovascular disease age-adjusted mortality rate since 2011 is perplexing (taken from Fig. 1A @BYan415 et al 2025 JACC). As @hmkyale writes, "our toolbox has grown: we now have more effective medications, robust trials, and clearer guidelines...[and] national spending on health care has reached unprecedented levels". Cardiovascular outcomes are not improving. His recent editor's page highlights the need to incentivize prevention and implementation. Can we coordinate care? Can we ensure patients can get their meds? There are MANY last mile problems that need to be tackled to ensure patients receive the care they need.
Risk factor control has plateaued too. @kfaridiMD et al 2025 JACC figure estimate population-wide 10-year risk from 2011-2020 using PREVENT equations (*). Risk plateaus around when mortality did for the US population. One takeaway is that further decreases in CVD mortality are preferentially to be had by decreasing risk (as opposed to developing new acute treatments for CV events). We have meds (statins, pcks9i, etc.) to decrease risk and many more coming (marea tx lipid drugs, verve/lilly LDL editing). How can we leverage those to ensure risk decreases? And subgroups within the population where risk is rising receive the meds/care they need? This is now primarily a problem in implementation not basic biology or drug discovery imo.
(*) We can estimate PREVENT 10-year risk from 2000-2010 to understand the relationship between population level risk and mortality when CVD mortality was decreasing. Scheurmann et al 2024 JAMA Netw Open uses NHANES data to externally validate PREVENT equations but a similar approach could be used to generate PREVENT 10-year risk for each cycle.
Thanks to @KTVU for covering our study on heart disease deaths in @JACCJournals
Takeaway #1: Let's address #highbloodpressure with the urgency and concerted effort that we showed towards combatting #smoking.
Takeaway #2: #Diet is a major cause - but one that we can change!
🚨Two new JACC Advances papers drop today linking SGLT2 inhibitors ↔ apolipoprotein M (ApoM) across very different settings—ambulatory HFrEF (DEFINE-HF) and acute inflammation (LPS-sepsis & COVID-19). Let’s unpack why this kidney-liver-vascular axis matters.
A 🧵
1️⃣/15
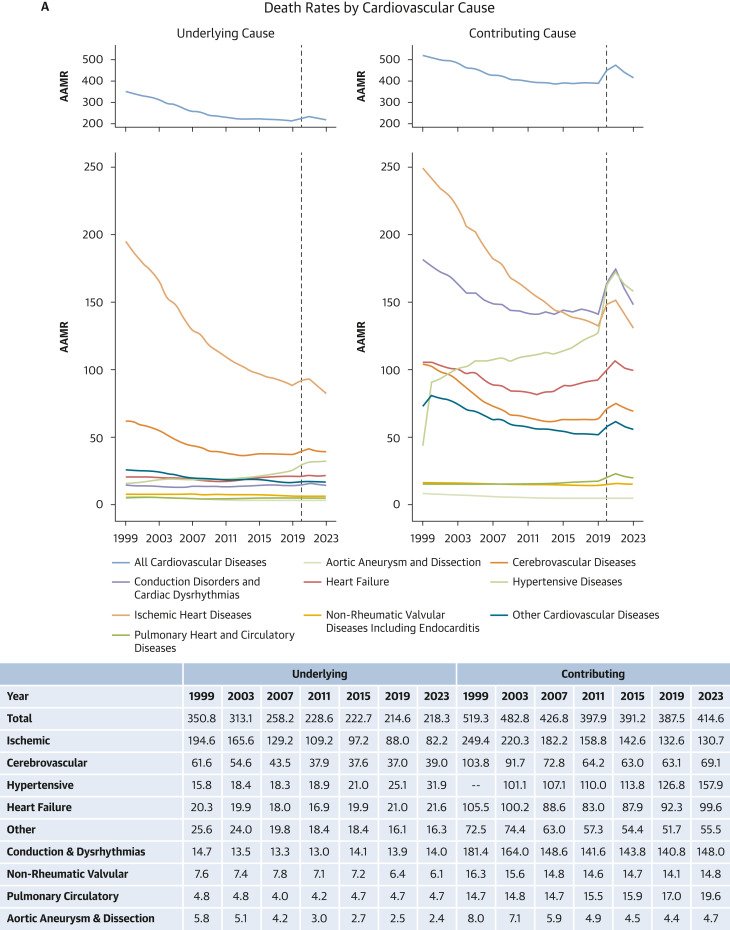
Our new study in @JACCJournals led by @BYan415 highlights that hypertension (as a primary cause of death) age-adjusted death rate doubled from 15.8 per 100,000 in 1999 to 31.9 in 2023. Striking given that overall cardiovascular mortality and basically all other sub-causes have declined in this 24 year interval. Hypertension as a contributing cause of death now has the highest sub-cause death rate at 157.9 in 2023 from 101.1 in 2003. We should dedicate more resources to figuring out why this is happening and how to reverse this trend.
In @JACCJournals, we report U.S. Deaths from #Hypertension have DOUBLED in rate since 1999
Deaths from #heartfailure and #stroke rising too
Good news? #COVID-era increases have fallen
Further efforts at #riskfactor control needed to save lives
More: https://t.co/j0jkp1mGhF














![aditharun_'s tweet photo. The timing of the observed plateau in cardiovascular disease age-adjusted mortality rate since 2011 is perplexing (taken from Fig. 1A @BYan415 et al 2025 JACC). As @hmkyale writes, "our toolbox has grown: we now have more effective medications, robust trials, and clearer guidelines...[and] national spending on health care has reached unprecedented levels". Cardiovascular outcomes are not improving. His recent editor's page highlights the need to incentivize prevention and implementation. Can we coordinate care? Can we ensure patients can get their meds? There are MANY last mile problems that need to be tackled to ensure patients receive the care they need.
Risk factor control has plateaued too. @kfaridiMD et al 2025 JACC figure estimate population-wide 10-year risk from 2011-2020 using PREVENT equations (*). Risk plateaus around when mortality did for the US population. One takeaway is that further decreases in CVD mortality are preferentially to be had by decreasing risk (as opposed to developing new acute treatments for CV events). We have meds (statins, pcks9i, etc.) to decrease risk and many more coming (marea tx lipid drugs, verve/lilly LDL editing). How can we leverage those to ensure risk decreases? And subgroups within the population where risk is rising receive the meds/care they need? This is now primarily a problem in implementation not basic biology or drug discovery imo.
(*) We can estimate PREVENT 10-year risk from 2000-2010 to understand the relationship between population level risk and mortality when CVD mortality was decreasing. Scheurmann et al 2024 JAMA Netw Open uses NHANES data to externally validate PREVENT equations but a similar approach could be used to generate PREVENT 10-year risk for each cycle.](https://pbs.twimg.com/media/GzOdStwX0AAugwo.png)



















![aditharun_'s tweet photo. The timing of the observed plateau in cardiovascular disease age-adjusted mortality rate since 2011 is perplexing (taken from Fig. 1A @BYan415 et al 2025 JACC). As @hmkyale writes, "our toolbox has grown: we now have more effective medications, robust trials, and clearer guidelines...[and] national spending on health care has reached unprecedented levels". Cardiovascular outcomes are not improving. His recent editor's page highlights the need to incentivize prevention and implementation. Can we coordinate care? Can we ensure patients can get their meds? There are MANY last mile problems that need to be tackled to ensure patients receive the care they need.
Risk factor control has plateaued too. @kfaridiMD et al 2025 JACC figure estimate population-wide 10-year risk from 2011-2020 using PREVENT equations (*). Risk plateaus around when mortality did for the US population. One takeaway is that further decreases in CVD mortality are preferentially to be had by decreasing risk (as opposed to developing new acute treatments for CV events). We have meds (statins, pcks9i, etc.) to decrease risk and many more coming (marea tx lipid drugs, verve/lilly LDL editing). How can we leverage those to ensure risk decreases? And subgroups within the population where risk is rising receive the meds/care they need? This is now primarily a problem in implementation not basic biology or drug discovery imo.
(*) We can estimate PREVENT 10-year risk from 2000-2010 to understand the relationship between population level risk and mortality when CVD mortality was decreasing. Scheurmann et al 2024 JAMA Netw Open uses NHANES data to externally validate PREVENT equations but a similar approach could be used to generate PREVENT 10-year risk for each cycle.](https://pbs.twimg.com/media/GzOe3d1XwAEN-R8.jpg)