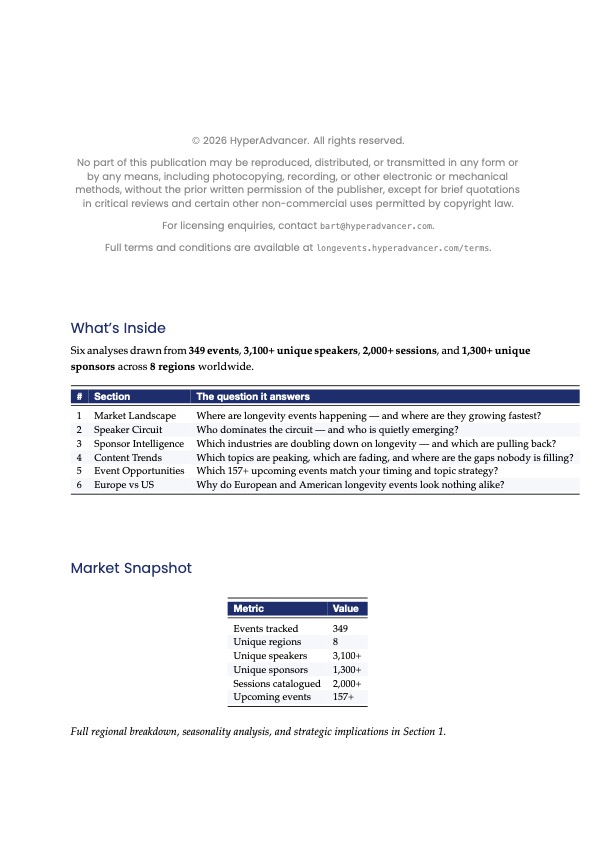
The Q1 2026 Longevity Events Intelligence Report is live.
349 events. 3,100+ speakers. 6 analyses. New this quarter: Europe vs US Regional Analysis.
Three findings:
1️⃣ EU peaks June + October (academic-led); US spreads year-round (C-suite-heavy)
2️⃣ 70 speakers active on both sides of the Atlantic
3️⃣ 66 events this quarter; North America 56%, Europe 23%, Asia 12%
https://t.co/9QJ24HWEKY
Mensen klagen dat er geen zekerheden meer in het leven zijn.
Dat kunnen artsen niet zeggen. Van zodra er begrotingsgesprekken aankomen, kan je er een fortuin op wedden dat er een artikel zal verschijnen over wat ze verdienen, waarbij appelen met peren worden vergeleken.
Uiteraard worden dit soort artikelen vanuit de politiek gestuurd. Laten we vooral niet naïef zijn. De wereld is klein 😉
P.S.: Het regent "afgunstartikelen" vandaag in de Vlaamse media. Miljonairs, Knokke-Heist, ....
@GevaertThomas@NDeMeurechy@MediSfeer@SGeysenbergh
https://t.co/4aqJfhQYRf
Tijdens een sessie van de Health Innovation School bouwde ik live een werkende app voor zo'n veertig zorgprofessionals. Zonder één regel code te typen. Eén prompt, paar minuten wachten, en iedereen kon het prototype meteen op de eigen smartphone gebruiken.
De reactie in de zaal zei genoeg: hier gebeurt iets fundamenteels.
Jarenlang gold dat zorginnovatie afhankelijk was van ontwikkelteams, projectplannen, budgetten en lange doorlooptijden. Dat klopt steeds minder. Met vibe coding beschrijf je in gewone taal wat je nodig hebt, en AI maakt er een werkend concept van. Niet productierijp, maar wel concreet genoeg om te testen, te verbeteren en veel scherper over te dragen aan echte ontwikkelaars.
De bottleneck verschuift daarmee. Niet techniek is het schaarse goed, maar domeinkennis. En die zit juist bij artsen, verpleegkundigen en paramedici op de werkvloer; zij weten precies waar processen wringen.
In oktober krijgt dit een vervolg met een clinical build day in België: zorgprofessionals bouwen samen met technische mentoren prototypes voor problemen uit hun eigen praktijk.
Consumenten wachten niet tot het zorgsysteem verandert. De vraag is niet meer óf je meebeweegt, maar hoe snel je zelf de eerste stap durft te zetten.
Mijn oproep aan zorgorganisaties: stop met radicale innovatie alleen bespreken. Ga zelf bouwen.
https://t.co/2OPBo49qcv
91% of people admit they keep scrolling even when they know they should stop. That number is worth sitting with.
PureGym mapped the damage literally: the average thumb travels 2.8km a week across a screen, so they built a 2.8km walk and called it a Joy Stroll. Neat creative reframing.
But the tension I keep returning to: gyms have a commercial interest in your anxiety. Low mood, poor sleep, restlessness are conversion drivers. So is this genuinely addressing the root cause, or just positioning the brand inside the mental health conversation without disrupting it?
Does the medium matter, or is any nudge toward movement net positive regardless of who's behind it?
The reason Ozempic makes you feel sick is also part of why it works. It slows your stomach to a crawl, so food sits there and you feel full for hours. Most people accept the nausea as the price of losing weight.
@novonordisk's next drug, zenagamtide, may break that trade. It hit 24% body weight loss over 36 weeks in people, and the new finding presented this month is what sets it apart: it appears to suppress appetite straight from the brain’s hunger circuits, without slowing the stomach at all.
The catch is that the no-slowed-stomach result is still early, shown in animals, not yet confirmed in humans. If it holds, the queasiness that makes people quit may fade, and the rule that you stop these drugs before surgery may stop applying.
The version of these drugs that skips the gut is the one to watch.
A very impressive study for how we could prevent lung cancer more than 5 years before it is diagnosed. Using machine learning, discovery of a 14-plasma protein signature of risk that predicts responsiveness to an antibody therapy to interleukin, IL-1β
Validated across 8 cohorts
@CellCellPress@CharlesSwanton
https://t.co/qpPtgs1dH0
@h4longevity please let me know when you decide on a concrete date for the 2027 event https://t.co/1z1TiOY9QX , that way i can add it to https://t.co/MqAIvX90hi thanks
@PieterVBO Terwijl dat de oorzaak van de hoge kostprijs elders ligt @PieterVBO : overmatige overhead en administratie (die trouwens ook zorgt voor de uitstroom uit het beroep, rechtstreeks en onrechtstreeks). https://t.co/xVWOE6IpJk
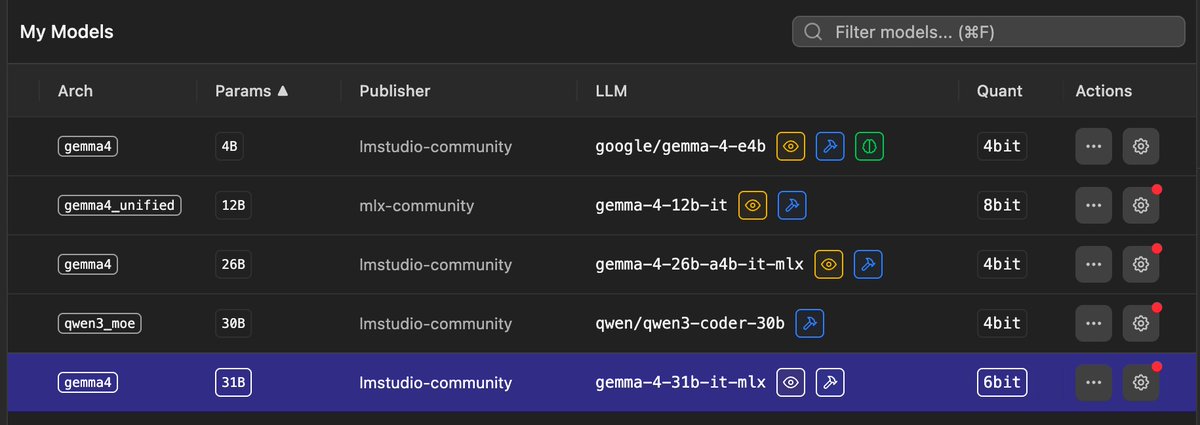
Claude Code auto swapping out models (optimising) in @lmstudio depending on the use case was a reveal to me. And now even better with the Gemma 4 12B model.
Extra benefit is that I can now sometimes use my laptop as an extra heater in my house 🤡
@vrtnws Zelden hoor je iets over de grootste oorzaak van de kostprijs : overmatige overhead en administratie (die trouwens ook zorgt voor de uitstroom uit het beroep, rechtstreeks en onrechtstreeks). https://t.co/1qjjHJBPgw
The model deploys first inside Mayo Clinic for continuous real-world testing before any wider release via Azure Foundry. That sequencing; live clinical environment before commercial rollout; is relatively rare for a frontier model and worth tracking as a validation approach.
The ownership structure here is the detail worth watching.
Mayo owns the model. Microsoft supplies compute, engineering, and AI capability. That's a different deal architecture than most health-tech partnerships, where the tech company retains the IP and the hospital becomes a reference customer.
The logic is clear: de-identified longitudinal clinical data is the scarce input. Mayo holds that. Microsoft holds the infrastructure. Splitting ownership accordingly makes sense.
What I'm less sure about: how "de-identified" holds up once a frontier model gets deployed at scale. Re-identification risk grows as models get more capable. Does owning the model also mean owning that liability?
New study of 111,646 women: GLP-1 use was linked to about 30% lower breast cancer incidence.
For scale, tamoxifen (the drug we prescribe to prevent it) runs about 38%, minus the endometrial cancer and clot risk.
Not proof yet, but looks very promising.
Uber reportedly now caps coding agents at $1,500/month per employee per tool - seems sensible to me, but it's also an interesting hint at the value Uber thinks these tools are providing
https://t.co/6YT0lCzPml
We just launched Sites into Codex!
Software creation was always about more than writing code. Sites in Codex fundamentally gives the power of end-to-end software creation to every user, no matter their technical fluency.
These Sites are fully deployed to a URL, private to workspaces, come with authentication, can have static files, and can store dynamic data in databases.
It is in preview for business and enterprise teams and will be rolling out to all workspaces over the next day. Give it a try by typing @ Sites into Codex and ask it to build anything!
This project took a massive amount of effort across hundreds of people at OpenAI - proud that we were able to get this out and excited to see what you all build with it!