I’ve never felt so much respect for someone in a floral fanny pack
Great @newsobserver photo of one of the many nurses on the front lines of this pandemic, at @UNC_Health_Care
1. One of formative experience of grad school for me was when our lab moved across the hallway to a bigger space & I realised my research didn’t really matter in the grand scheme of science & that this actually made me love science even more. So here is a thread about that.
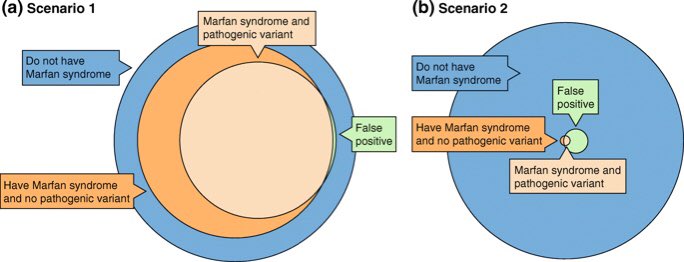
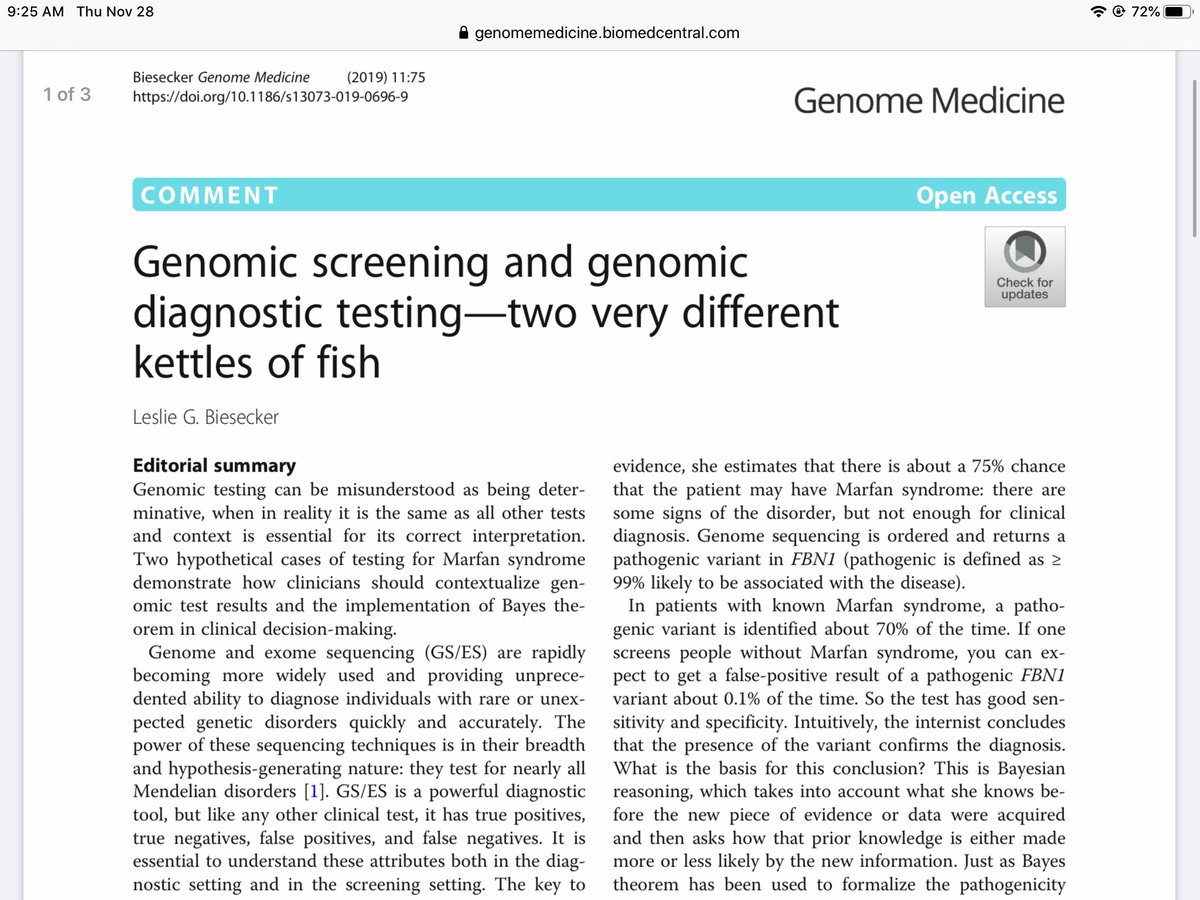
“Bayes theorem applies to everything clinicians do:” Les Biesecker writes in @GenomeMedicine about the simple but fundamental difference between genomic screening and genomic diagnostic testing. https://t.co/lUgnYjk0xw
@UNC_SOM also emphasizes SDofH, and students are actively engaged with underserved populations. They also do need to learn about modern technology and be part of the discussion about how/when it can/should be applied. Not saying they should sequence their own genomes though...
@cecilejanssens We have a required full term course on social determinants of health and health disparities @bcmhouston As a geneticist totally agree with you that is more important than @EricTopol suggestion of everyone sequencing their genome.
@jwbelmon When I see this I think:
1) some of these assertions may be wrong (how good is the supporting evidence?)
2) some of these might actually be part of the same phenotypic spectrum and not distinct disorders (lumping vs. splitting)
3) pleiotropy and variable expressivity are cool!
@A_Elhabyan@ClinGenResource Volunteers can complete a questionnaire here: https://t.co/IdGVjl9xIa
It will get some info about your background and your interests, and then ClinGen staff will match you up with opportunities to contribute as a curator.
Use of genomic screening in newborns and children requires careful thought about what information to include. NC NEXUS used "age-based actionability" to help categorize conditions for parental decision-making. https://t.co/bZkWWExS4f @NICHD_NIH @UNCResearch
Who knew people could mis-use genetic tests? 🙄
Any guesses as to what "genetic condition" this guy was diagnosing based on 23andMe in order to gain exemptions? MTHFR, anyone? https://t.co/vFnGkFLahs #psuedoscience#pseudomedicine
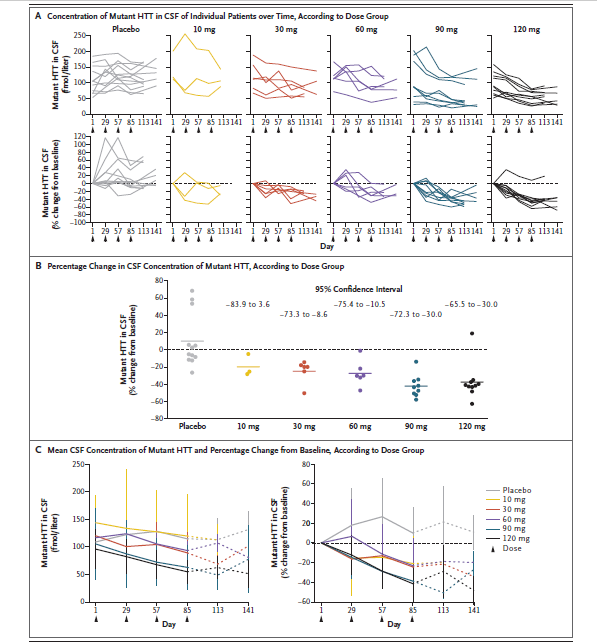
Cautiously optimistic about therapeutic intervention in Huntington disease. Exciting to see reduction in mutant HTT in CSF after intrathecal antisense oligo, but looking forward to Phase 2/3 trials studying outcomes & prevention of manifestations.
@RobertCGreen@TheACMG@RobertCGreen do you agree that if @TheACMG were going to make recommendations about population screening they would likely need to use a very different process than the one that was used for secondary findings?
The distinction is between what genes were deemed by the ACMG Secondary Findings working group to be important enough to look for when someone undergoes clinical genomic sequencing for diagnostic purposes, versus those that should be actively sought in the general population.
Haven't read the book, but quotes from the review ("geneticist Robert Plomin ...presents DNA as a “fortune-teller” that is “100 percent reliable” and that can “predict your future from birth”) make me cringe. Hard to fathom anyone making claims that mutilate our science this way.
"No matter how good our understanding of the genetics of intelligence gets, we will never be able to predict intelligence of individuals with accuracy from genomic information." says @WiringTheBrain
Never accurate. Not even close.
https://t.co/6wULtGFCHS
@dannydesloover The question is about who you target your interventions to, before they get obese. If you just pick the top decile you will fail to intervene on the majority of kids who will become obese. A population-level program would target everyone for a more healthy lifestyle.
The problem with focusing intervention on the top decile of PRS is that it would ignore the majority of kids who will be overweight, obese, or severely obese, but who have a "normal" PRS (~82%, 79% and 68%, respectively)...
@GENES_PK@WBUR Is your suspicion population-level programs > impact than targeting high genetic-risk kids
based on
evidence (i.e., proven efficacy of population-level programs for obesity) or just a hypothesis?