During yesterday’s WHO checklist in the EP lab I tried to confirm with the patient what procedure he was expecting. He was thought he was getting an abomination. #EPeeps
Getting a chance to play with Medtronic’s new Nitron console, making the CryoPVI experience even smoother. Theo Nikolaidou performed the worldwide first case this morning then my turn this afternoon!
Photographer Daniel Antoniol employs an innovative approach to alter perspective, giving the illusion that the moon is being transported
📸daniel_antoniol
@Irina67790690@ecgrhythms If the RV/RA is on the right side of the image (looks like a flipped 5 chamber view with the AV and LVOT on the left) there appears to be apical displacement of the tricupid valve leaflets which would make this Ebstein’s anomoly.
@DaveRichley@ecgrhythms Grouped beating, looks like Wenckebach with some variation in PP interval. Some p-waves appear as pseudo-R’ waves in V1. PP appears longer when there isn’t a QRS between Ps. Suggests ventriculophasic modulation.
@smithECGBlog@ecgrhythms If conventional DCCV fails, also consider other manoeuvres like AP pad position, compressing chest during defib, and even double sequential defibrillation https://t.co/omZODG79Le
@syamkumarmd@ProfErkanBaysal Differential diagnoses
(1) Dual AV nodal physiology with simultaneous conduction down fast and slow pathways of the AV node giving a two-for-one ventricular response
(2) Frequent extrasystoles arising from the His with retrograde block to the atria
@shahinzamanii@echo_batman The pre-excitation is intermittent, and the T-wave inversion mentioned is not present on the non-pre-excited beats. QRS complexes of this amplitude may well be a normal finding in a 16y M. Certainly echo, but could well be a structurally normal heart.
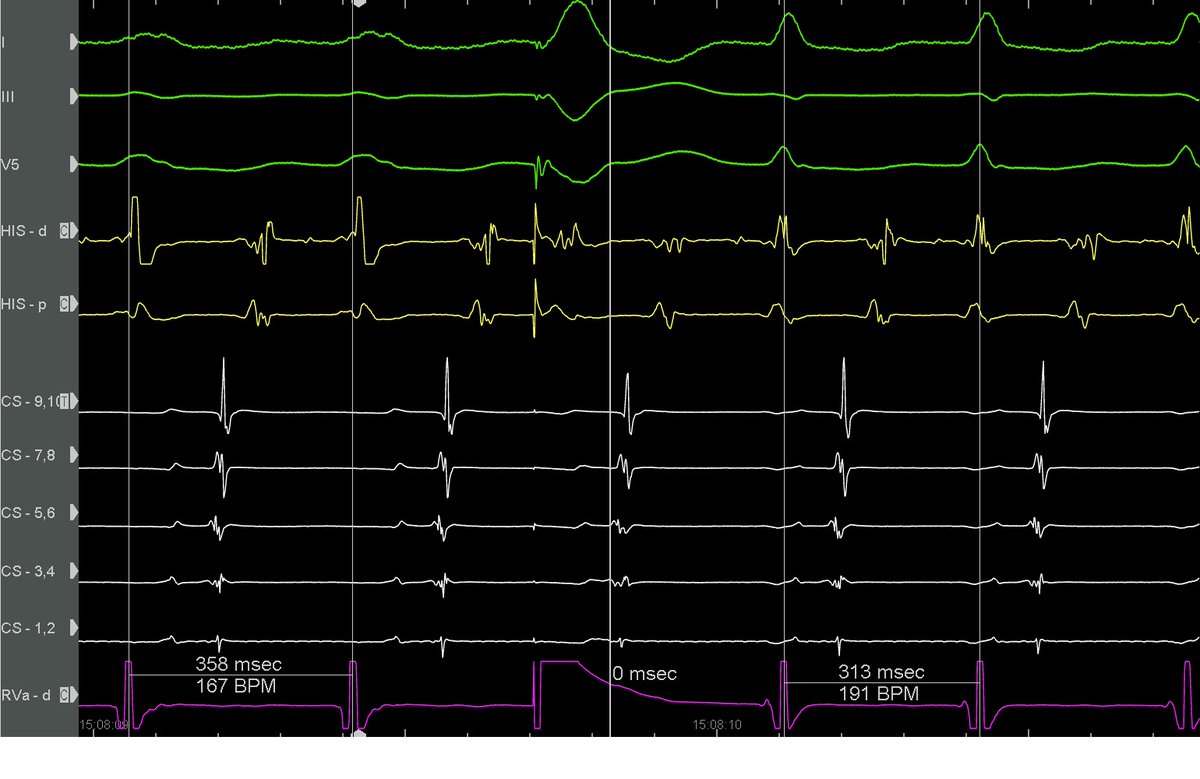
Importance of rapid pacing to achieve 2:1 block during retro mapping of concealed PS AP. Looking at last 2 beats difficult to be sure where retro A starts, but with isolated V clear that it starts at red line (early) not blue (late c/w CS 7,8). Not new but worth reminder IMHO.
@KasparHauser15@RobertHermanMD You’re right - most pre-excited beats are ‘fused’ as a combination of conduction through accesory pathway and AV node. Changes in QRS morphology can be caused by the relative contributions of conduction through the two e.g slower conduction through AVN -> greater pre-excitation