Tratamos la disfunción autonómica integrando neurociencia, inmunología y metabolismo para devolver el equilibrio a tu cuerpo. 🌀
🔬 Ref: Frontiers in Behavioral Neuroscience, 2026. PMID: 42328360.
https://t.co/JQdIUQbTxl
#Disautonomía#CovidPersistente#Neuromodulación
Un nuevo modelo demuestra que las células inmunitarias humanas promueven la diseminación multiorgánica del #SARSCoV2 y que las células T humanas limitan la inmunidad innata antiviral.
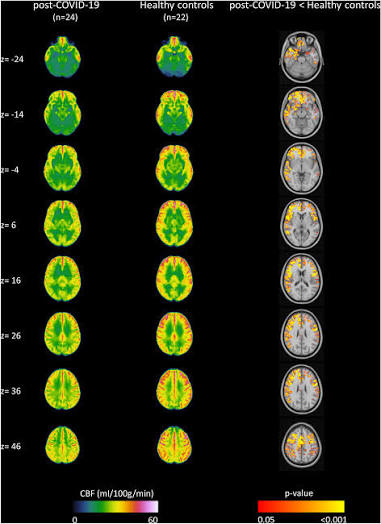
Brain Fog is a main symptom in Long Covid Patients. Autonomic Reflex Dysregulation leading to a failure of Cerebral Autoregulatory Pathways that maintain constant levels of blood in the brain during exertion and changes in position. Notice in the cadaver brain the difference between Normal blood flow vs Long Covid inadequate blood flow. #LongCovid #pwME #POTS #Dysautonomia #pwLC
Y aquí es donde le duele a la economía
"Absentismo laboral"
"El incremento de las bajas complica la actividad en pequeños negocios"
Ni que estuviera circulando un virus vascular, multisistémico, inmunosupresor y neurotrópico con incontables estudios sobre sus daños a la salud
NIH press release:
"Immune system may attack nervous system in some Long COVID patients"
https://t.co/Ga7Ycuxg3F
Paper:
A causal link between autoantibodies and neurological symptoms in long COVID
https://t.co/nPYwvjhLAo
#LongCovid
SARS-CoV-2 disrupts the TFEB-autophagy-lysosome pathway, a system critical for antigen processing, interferon responses, and immune homeostasis. If true, this provides a plausible mechanism by which antigen-presenting cells become chronically dysfunctional long after acute infection has resolved. An upstream mechanism from APC dysfunction. 😱
https://t.co/0j1O85fqTK
🚨Long COVID is linked to lasting sleep problems, including unhealthy sleep duration, poor sleep quality, and sleep disturbance, nearly 3 years after initial infection.
So, Covid-19 can add an extra #HealthRisk for multiple chronic conditions and mortality!
Thanks, David!
🌀🧠🌀SENSIBILIZACIÓN CENTRAL EN LA COVID PERSISTENTE: DISAUTONOMÍA, HIPOPERFUSIÓN CEREBRAL Y NEUROINFLAMACIÓN
🧵1⃣🇺🇸Artículo de 2 neurólogos de Mass General Brigham, Facultad de Medicina de Harvard
https://t.co/umqE16SWFV
Sobre el daño genético Sars2
✴️👶🧬LAS CITOCINAS PATERNAS ALTERAN EL ARN DEL ESPERMA ASÍ COMO EL CEREBRO Y COMPORTAMIENTO DE LA DESCENDENCIA
🧵1⃣🦘Artículo de 6 Neurocientíficos de Instituto Florey de Neurociencia y Salud Mental y Univ de Melbourne
https://t.co/Ss4fTgnHIN
Se ha observado una asociación prospectiva entre la #CoVID19 y problemas de sueño tres años después de su inicio. Es necesario mejorar la salud del sueño en las personas con #LongCoVID. https://t.co/Za2NMEqq98
⚠️💊 Long COVID and ME/CFS: a layered strategy, not a single treatment for everyone
One of the mistakes when talking about Long COVID and ME/CFS is looking for “the treatment”, as if all patients had exactly the same mechanism.
They do not.
But that does not mean there is no common logic.
The model I propose is to think of these diseases as post-infectious processes maintained by layers:
A persistent pathogen or a sustained antigenic source.
Chronic immune hyperactivation.
Immune exhaustion and poorer control of latent pathogens.
Secondary reactivations that add more antigenic load.
Systemic consequences: inflammation, mast cells/histamine, oxidative stress, barrier dysfunction, autoimmunity, dysautonomia, neuroinflammation, endocrine alterations or vascular involvement.
Baseline treatments and then treatments directed according to the dominant mechanism.
The key is not to place all layers at the same level.
Not everything is a primary cause.
Some things are consequences.
And some consequences, once they appear, can become amplifiers that maintain the vicious cycle.
Long COVID and ME/CFS: same model, different degree of classification
For me, Long COVID and ME/CFS are not opposite processes.
They may follow the same post-infectious model.
The main difference is that Long COVID is better classified by its initial pathogen: SARS-CoV-2.
By contrast, ME/CFS is a more heterogeneous label where post-infectious patients initiated or maintained by different pathogens may be grouped together: EBV, HHV-6, CMV, enteroviruses, parvovirus B19, Borrelia, Toxoplasma or other persistent, latent or intracellular pathogens.
In other words:
Long COVID would be a post-infectious disease defined by SARS-CoV-2.
ME/CFS could include several similar post-infectious subtypes, but initiated by different pathogens.
The underlying logic would be the same:
persistent pathogen or antigenic reservoir
→ continuous immune stimulation
→ chronic immune hyperactivation
→ sustained inflammation
→ T/NK cell exhaustion
→ poorer control of latent pathogens
→ new reactivations
→ more antigenic load
→ more inflammation.
Therefore, the problem would not be that Long COVID and ME/CFS have nothing to do with each other.
The problem is that ME/CFS probably mixes post-infectious patients of different origins under the same clinical label.
▪️Long COVID: SARS-CoV-2 as the initial persistent source
In Long COVID, the initial axis would be the persistence of SARS-CoV-2 in tissue or cellular reservoirs, with sustained or intermittent production of viral antigens.
There does not necessarily have to be detectable viremia in blood.
But if the immune system keeps seeing viral antigens months or years later, those antigens are not well explained as simple passive “remnants” from the initial infection.
The body degrades proteins and RNA through proteases, nucleases, autophagy, the proteasome, cellular turnover and immune clearance.
For this reason, prolonged presence of viral antigen points to a sustained source:
tissue reservoirs;
infected cells;
low-level persistent infection;
abortive or incomplete infection;
intermittent production of viral material;
local reactivation;
or cellular persistence in tissues where the immune system does not properly eliminate the stimulus.
In other words:
if there is persistent antigen for months or years, we need to think of some type of reservoir or biological source that renews it.
That stimulus keeps the immune system chronically activated.
And that chronic activation can lead to persistent inflammation, immune exhaustion and poorer control of other latent pathogens.
Un equipo internacional de 60 expertos de 10 países, con participación destacada de investigadores de la REiCOP (@_REiCOP), ha publicado la primera guía internacional de práctica clínica centrada en la prevención y tratamiento de la #COVIDPersistente en adultos.
¿Qué tienen en común la niebla mental, la intolerancia ortostática, el dolor generalizado y la fatiga extrema? 🧠
Un estudio apunta a que podrían estar conectados por un mismo mecanismo neurobiológico: la sensibilización central.
Hilo 🧵
Chosun University, 629 adults with Long COVID.
Four symptom profiles emerged.
Fatigue and post-exertional malaise were most severe, while heavier multisystem symptoms tracked with poorer quality of life.
https://t.co/fKgOHFx7kK
Estudian la sangre de personas con Covid persistente y encuentran estructuras anómalas que no deberían estar ahí | Fernanda Tapia https://t.co/Kv7dqcBDZm
Hoy en nuestro #15alas15 la compartimos el vídeo del programa @fiestatelecinco de @fiestatelecinco donde algunos Pacientes de Covid Persistente cuentan como no han vuelto a la normalidad tras haber pasado el Covid y nos ha dejado indefensos ante una nueva enfermedad en la que nos hemos tenido que defender y luchar solos
Pero no todo lo podemos hacer solos, necesitamos ayuda de las intituciones, entre otras cosas en: más investigación, acceso a tratamientos sin importar el código postal o el hospital de referencia y una adecuada revisión de las discapacidades e incapacidades o en su defecto una correcta adapatación laboral.
🫠 Tras 6 agotadores años, se nos acaban las fuerzas!!!
Difunde y ayúdanos no sólo a ser más conocidos sino también a encontrar ayuda de las instituciones 🙏
@CasaReal@sanidadgob@SaludMadrid@EU_Commission@GobiernoEs@Monica_Garcia_G@IdiazAyuso@FatimaMatuteCM@ComisionEuropea
#longcovidawereness #longcovidmakesusone #covidpersistente #EndTheSilence
¿Y si aumentar la disponibilidad de oxígeno pudiera ayudar a "reconfigurar" circuitos cerebrales alterados en la EM/SFC?
Nuevo estudio de la Dra. Carmen Scheibenbogen (@C_Scheibenbogen ) y colegas:
Abro hilo 🧵
Más sobre el daño cerebral Sars2
⚡️🧠⚡️COVID19: LESIÓN INFLAMATORIA DEL PEDÚNCULO CEREBRAL QUE SE MANIFIESTA COMO ESPASMOS TÓNICOS DOLOROSOS
🧵1⃣🇺🇸Artículo de 3 neurólogos de la Universidad de Stanford
https://t.co/vGex5bhfIR