🫀 Pulmonary Vein PW Doppler: A Hidden Gem in Diastology
Pulmonary vein pulsed-wave Doppler provides valuable insights into left ventricular filling pressures, left atrial function, and mitral regurgitation severity.
📍 How to Perform Pulmonary Vein PW Doppler?
Thread 👇
📚 Según el consenso internacional, existen tres tipos principales de Válvula aórtica bicúspide:
1️⃣ VAB con fusión completa de cúspides
2️⃣ VAB de dos senos
3️⃣ VAB con fusión parcial de cúspides, también llamada forma frustrada
🏃♂️ Elevated troponin after exercise… should we worry?
💥 Cardiac troponin = gold standard for myocardial injury.
👉 But what happens after intense exercise?
📊 A large meta-analysis (129 studies, >7,000 athletes) shows:
➡️ 36% of athletes have troponin levels above the normal limit after exercise
⚠️ That’s more than 1 in 3.
🔬 Key determinants (see Graphical Abstract, page 3):
✔️ High-sensitivity assays → detect more elevations
✔️ cTnT > cTnI
✔️ Peak in endurance sports (running, cycling, triathlon)
✔️ Highest after 3–6 hours of exercise
📈 The curve on Figure 4 (page 29) shows a clear peak around 4–5 hours of effort.
👀 What DOESN’T matter (as much as we thought):
❌ Sex
❌ Training status
👉 It’s not about who you are…
👉 It’s about what and how long you do.
🧠 Clinical dilemma:
Troponin ↑ = myocardial injury
BUT
Exercise alone can cause it
👉 So… how do we interpret it in the ER after a marathon?
💡 Take-home message:
🩺 Context is everything
👉 Consider exercise type, duration, and assay used
👉 Not every troponin rise = pathology
🚀 This is a perfect example of why biomarkers need clinical interpretation, not just thresholds.
#Cardiology #SportsCardiology #Troponin #Biomarkers #Endurance #ExercisePhysiology #CardioImaging #PrecisionMedicine #Athletes #Research 🏃♂️🧬
INSUFICIENCIA CARDÍACA CON FE PRESERVADA
🔴50% de los pacientes hospitalizados con ins. cardíaca tienen #HFpEF
-Diagnóstico:
🔴Síntomas
🔴FE ≥50%
🔴Evidencia de anormalidades estructurales o funcionales consistentes en disfunción diastólica y/o aumento presiones de llenado ventriculares, incluyendo el aumento de péptido natriurético atrial
-Tratamiento:
🔴Diuréticos 👍
🔴iSGLT-2 👍
🔴MRA, SRAA, Betabloq. ⏩Según comorbilidades
🔴GLP y GIP a. 🤔
Vía @ESC_Journals
https://t.co/VZWXWpxR8G
🫀Valvular cardiogenic shock is probably one of the most underrecognized phenotypes of shock in modern cardiac critical care.
What makes this paper particularly important is that it reframes severe valve disease:
not as chronic structural cardiology, but as acute hemodynamic catastrophe.
The physiology is brutal.
Unlike classic ischemic CS, VCS often combines:
🫀 abrupt preload overload
🫀 severe afterload mismatch
🫀 elevated filling pressures
🫀 pulmonary edema
🫀 impaired forward flow
🫀 rapidly collapsing ventriculo arterial coupling
And unlike MI related shock: 📌 many of these patients still have relatively preserved LVEF.
Which means: normal or “acceptable” EF does NOT exclude severe shock physiology.
One of the most fascinating findings: 📌 the aortic valve was the most commonly involved valve.
Especially: • aortic stenosis • acute aortic regurgitation
And outcomes differed substantially by lesion type.
Patients with:
⚠️ stenotic lesions had the worst survival
⚠️ regurgitant lesions performed better
⚠️ mixed lesions remained intermediate
Severe AS in shock creates:
• fixed forward flow obstruction
• catecholamine inefficiency
• coronary hypoperfusion
• profound ventriculo arterial uncoupling
while acute regurgitant lesions may still preserve some forward stroke volume if rapidly corrected.
Another extremely important message:
📌 definitive intervention mattered enormously.
Compared to medical therapy alone:
• surgery had the best survival
• percutaneous therapies were intermediate
• medical management had the worst outcomes
After multivariable adjustment: medical management alone was associated with nearly 4 times higher hazard of death at 1 year.
But this study suggests: ⚡ definitive therapy may be the only real survival strategy.
The paper also highlights something increasingly relevant for modern CICUs:
📌 prosthetic valve dysfunction accounted for almost one third of VCS cases.
With aging populations and expanding TAVR/bioprosthetic use: this phenotype will likely increase dramatically over the next decade.
From a hemodynamic perspective, VCS may require:
🩺 earlier invasive monitoring
🩺 advanced echocardiography
🩺 rapid valve team activation
🩺 individualized MCS strategy
🩺 faster transfer to high volume structural centers
The study also indirectly supports something many intensivists already suspect:
📌 timing is probably everything.
Delayed recognition likely converts salvageable hemodynamic collapse into irreversible multiorgan failure.
This is where future research should probably focus:
• shock phenotyping by valve lesion
• optimal MCS selection
• VA coupling analysis
• transcatheter rescue timing
• CICU to structural heart pathways
• predictive models for intervention candidacy
📖 Nair RM, JACC Advances. 2024;3(11):101303.
https://t.co/eo9wstNwiZ
Reading transmitral Doppler
The transmitral inflow pattern is one of the most fundamental windows into left ventricular diastolic function, filling pressures, and relaxation physiology.
After aortic valve closure, the LV begins to relax, but both valves remain closed during the isovolumic relaxation time (IVRT). During this phase, LV pressure falls rapidly without any change in ventricular volume.
Once LV pressure drops below left atrial (LA) pressure, the mitral valve opens and ventricular filling begins.
The first peak is the E wave (early diastolic filling).
This represents passive LV filling, driven by the pressure gradient between the LA and the relaxing LV. In healthy young adults, E velocity is typically dominant because ventricular relaxation is efficient and suction is preserved.
After the E-wave peak, flow slows as the LA-LV pressure gradient declines. This creates the deceleration slope, and the time from peak E to baseline is the deceleration time (DT), an important marker of LV compliance and filling pressure.
A brief phase of minimal flow may follow: diastasis, where LA and LV pressures nearly equalize.
The second peak is the A wave, generated by atrial contraction (atrial kick), which contributes to late ventricular filling.
Key quantitative parameters from transmitral Doppler:
🛑E velocity: peak early filling velocity
🛑A velocity: peak atrial filling velocity
🛑E/A ratio: quick assessment of diastolic filling pattern
🛑IVRT: time from aortic valve closure to mitral valve opening; reflects LV relaxation
🛑DT (deceleration time): reflects LV compliance and filling pressure
🛑VTI (velocity-time integral): total blood flow contribution during filling
🛑DFP (diastolic filling period): duration of ventricular filling
Clinical interpretation:
- A reduced E wave with dominant A wave (E/A <1) often suggests impaired relaxation.
- A very tall E wave with short DT may indicate elevated LV filling pressures and restrictive physiology.
- A seemingly normal E/A ratio can be deceptive (pseudonormal pattern), this is why tissue Doppler and LA assessment matter.
Transmitral Doppler is not just a waveform, it is a hemodynamic conversation between the left atrium and left ventricle.
Ref: Otto Catherine clinical textbook
🚨 ¿Cómo tratar la congestión en Insuficiencia Cardíaca Aguda (ICA)?
Un nuevo meta-análisis en el @EHJ_CardioPharma analiza 25 ensayos clínicos (7,149 pacientes) para darnos respuestas claras sobre las estrategias diuréticas. 🏥💊
مريض قلب وعنده عوامل خطورة كثيرة
تشخص ب UTI وراح يجيك تساؤل عن ادوية ال SGLT-I هل نوقفه او لا ؟!
افضل ارتكل خيالية راح تجاوب على هذا التساؤل لان المشكله ذي شائعه بالعيادات!
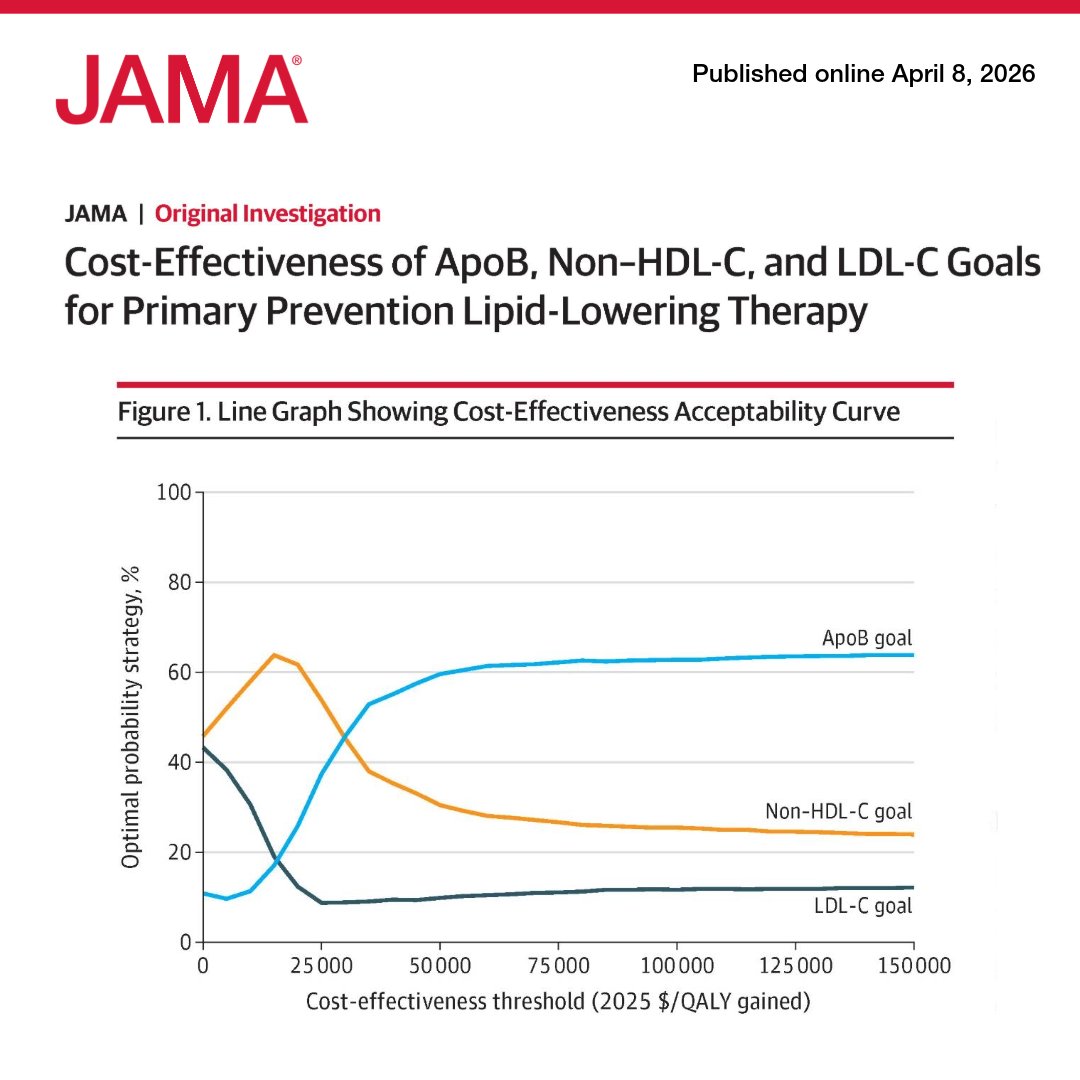
A computer simulation found #ApoB-guided intensification of lipid-lowering therapy provides the most QALYs and is highly cost-effective compared to #LDL-C or #nonHDL-C targets.
https://t.co/hu4lgTeKxV
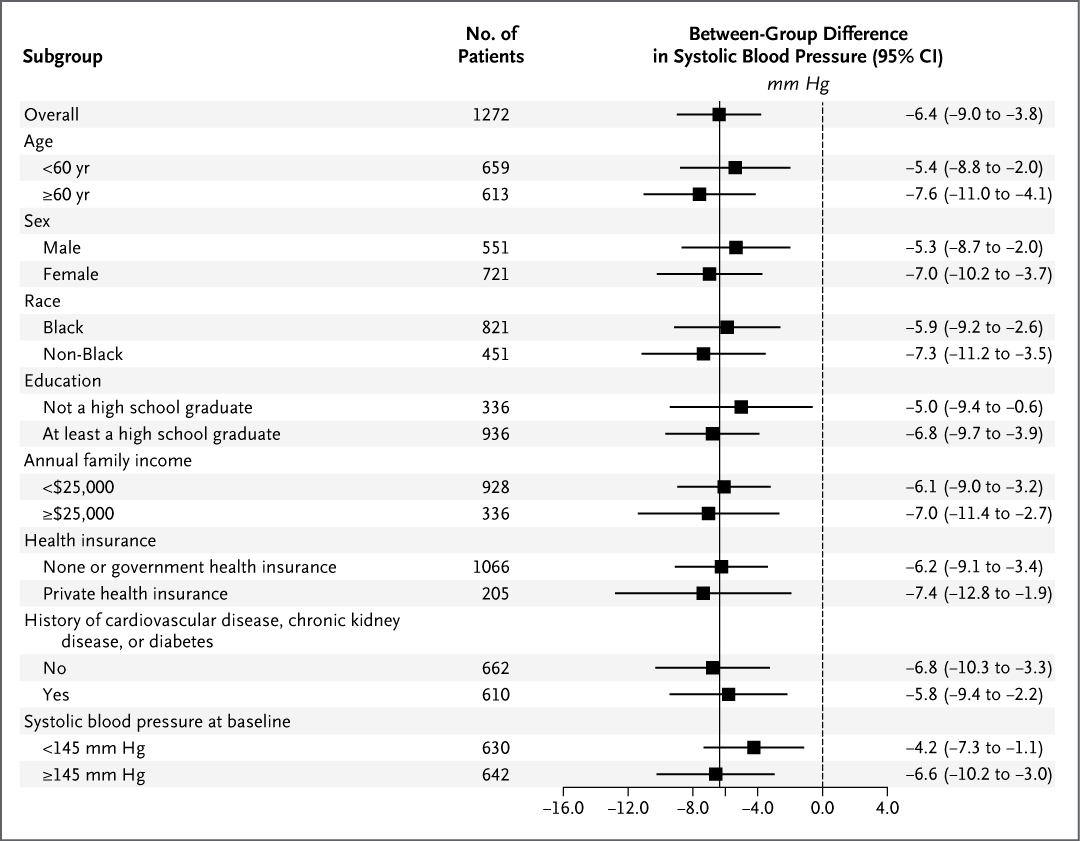
Original Article: Multifaceted Strategies for Hypertension Control in Low-Income Patients (IMPACTS-BP trial) https://t.co/AxUONCq718
Editorial: Systems-Based Success for Hypertension https://t.co/4BkINWpImo
#Cardiology
Among patients with anterior myocardial infarction, adding low-dose rivaroxaban to dual antiplatelet therapy did not significantly reduce left ventricular thrombus formation at 1 month but increased minor bleeding.
https://t.co/TDDR0p8sWV
🔰Acoplamiento ventrículo–arterial derecho (VD–AP) parámetro clave en la evaluación de la función del ventrículo derecho🫀
☕️Notas cafeteras.
“RV protective” (protección del ventrículo derecho) es una estrategia de manejo ventilatorio y hemodinámico diseñada para:
↪️ Evitar el desacoplamiento VD–arteria pulmonar y prevenir falla del ventrículo derecho.
☝🏻🤓En patologías como el SDRA:
▪︎La ventilación mecánica
▪︎La hipoxemia
▪︎La hipercapnia
👉 ⬆️Aumentan la resistencia vascular pulmonar (poscarga del VD)
➡️ Esto puede llevar a:
Dilatación del VD
↓ gasto cardíaco
↓ DO₂ sistémico
Shock
📌 Por eso nace el concepto:
🧠 No solo proteger el pulmón (lung protective)… sino también proteger el VD (RV protective)‼️
🎯 El acoplamiento ventrículo-arterial derecho representa un cambio de paradigma:
● Pasamos de evaluar “función del VD” → a evaluar su eficiencia energética frente a la carga pulmonar
👉 Es un parámetro: Fisiológico, integrador, pronóstico, accionable en UCI.
📌El acoplamiento ventrículo-arterial derecho (VD–AP) describe la relación entre la contractilidad del ventrículo derecho (VD) y la poscarga impuesta por la circulación pulmonar. Es un concepto derivado de la fisiología presión-volumen, donde:
▪️Ees (elastancia ventricular) = contractilidad del VD🫀
▪️Ea (elastancia arterial pulmonar) = carga vascular pulmonar🫁
👉 El cociente Ees/Ea define el grado de acoplamiento.💥
📌 Fisiología clave
🫀Un VD óptimamente acoplado transfiere energía eficientemente a la arteria pulmonar.
📚El valor ideal de acoplamiento:
🔰Ees/Ea ≈ 1.5–2 → eficiencia máxima🤗
🔰Ees/Ea < 0.8 → desacoplamiento (fallo del VD)😵💫
🫁 Importancia en el paciente crítico
🫀El VD es altamente sensible a cambios en la poscarga. En escenarios como:
▪️SDRA
▪️Tromboembolia pulmonar
▪️Hipertensión pulmonar
▪️Ventilación mecánica (↑ presión intratorácica)
▪️Sepsis con disfunción miocárdica
👉 El desacoplamiento VD–AP es un marcador temprano de fracaso hemodinámico antes de la caída del gasto cardíaco.🫀
⚖️Métodos de evaluación
1️⃣. Método gold standard (invasivo)
Bucles presión-volumen del VD
Medición directa de Ees/Ea
2️⃣. Métodos no invasivos (ecocardiografía crítica)
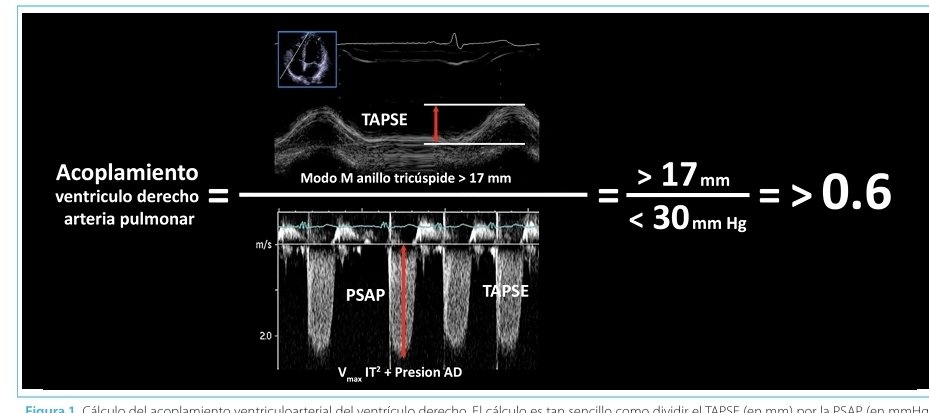
🔹 TAPSE/PASP
▪️TAPSE = excursión sistólica del anillo tricuspídeo
▪️PASP = presión sistólica pulmonar
👉 TAPSE/PASP ≈ surrogate de Ees/Ea.
TAPSE/PASP es un “surrogate” de Ees/Ea
➡️ Porque no mide directamente el acoplamiento, pero se correlaciona bien con él.
▪️> 0.31 mm/mmHg → buen acoplamiento
▪️< 0.31 → desacoplamiento VD–AP
🔹 S’/PASP (Doppler tisular)
💥Alternativa más sensible en algunos escenarios.
🔹 RV free wall strain / PASP
🫀Más precoz para detectar disfunción subclínica
🫀El acoplamiento VD–AP no debe verse aislado, sino como parte de la coherencia hemodinámica global:
▪️VD desacoplado → ↓ flujo pulmonar → ↓ retorno al VI
▪️↓ DO₂ sistémico → hipoperfusión tisular
▪️↑ presión venosa → congestión sistémica (VExUS positivo)
📍 1. SDRA
●PEEP alta → ↑ Ea → riesgo de desacoplamiento
●TAPSE/PASP permite ajustar ventilación “RV protective”
📍 2. Tromboembolia pulmonar
●Aumento súbito de Ea
●Desacoplamiento predice mortalidad
📍 3. Sepsis
●Miocardiopatía séptica → ↓ Ees
●Evaluar acoplamiento evita sobrecarga hídrica.
📍 4. Ventilación mecánica
●Driving pressure alta → impacto en VD
●Integrar con mecánica respiratoria
💎 PERLAS CAFETERAS ☕️
📣¿Qué implica una estrategia RV protective?
🎯Es un enfoque que modifica la ventilación para no dañar el VD
🔰Objetivos principales:
1. Reducir la poscarga del VD
⚠️Evitar:
▶️Hipoxemia
▶️Hipercapnia
▶️Acidosis. ....aumentan la resistencia pulmonar ‼️
2. Limitar presiones ventilatorias:
▶️Plateau pressure < 26–27 cmH₂O
▶️Driving pressure < 15 cmH₂O
👉 Altas presiones → ↑ presión pulmonar → sobrecarga del VD
3. Ajuste cuidadoso de PEEP
Evitar:
▶️Atelectasia (↑ poscarga)
Sobredistensión (↑ poscarga)
👉 El problema no es solo la PEEP…cont.
Manejo de Hemorragias en Pacientes Bajo Anticoagulación 🩸💊
🔰📚Acute Cardiovascular Care 2026
https://t.co/9AkjsSS2IK
Enlace a Articulo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
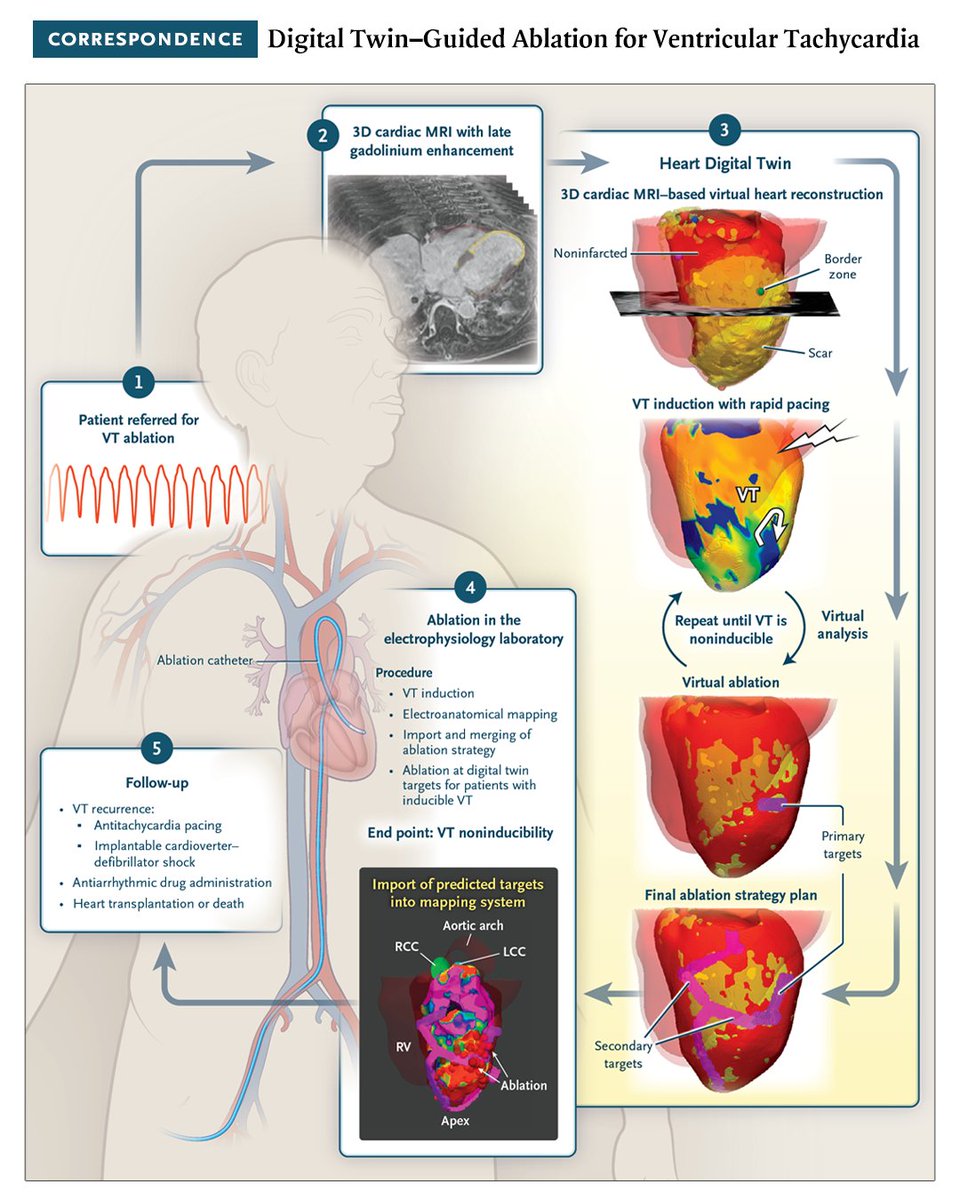
In a 10-patient feasibility study, heart digital twins were used to guide VT ablation. Afterward, VT was noninducible in all patients; at a mean follow-up of 13 months, 8 patients were free of recurrence, without drug therapy. Full study results: https://t.co/EyF2pI5pyI