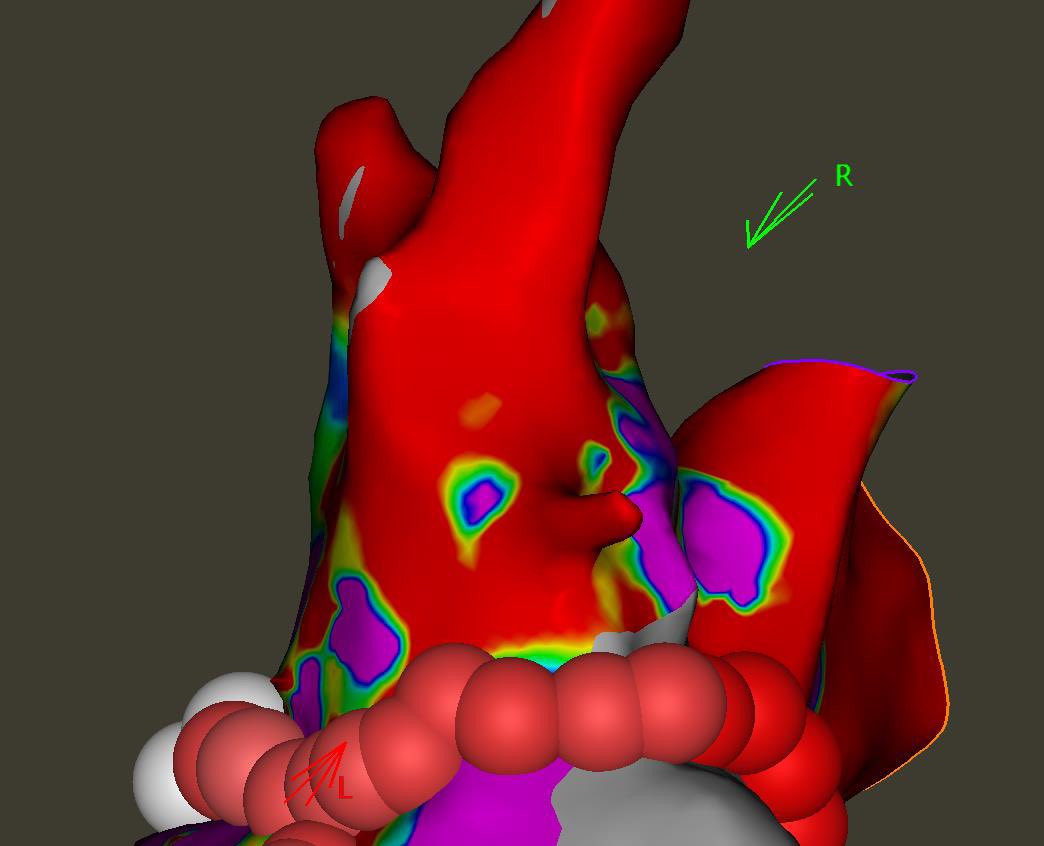
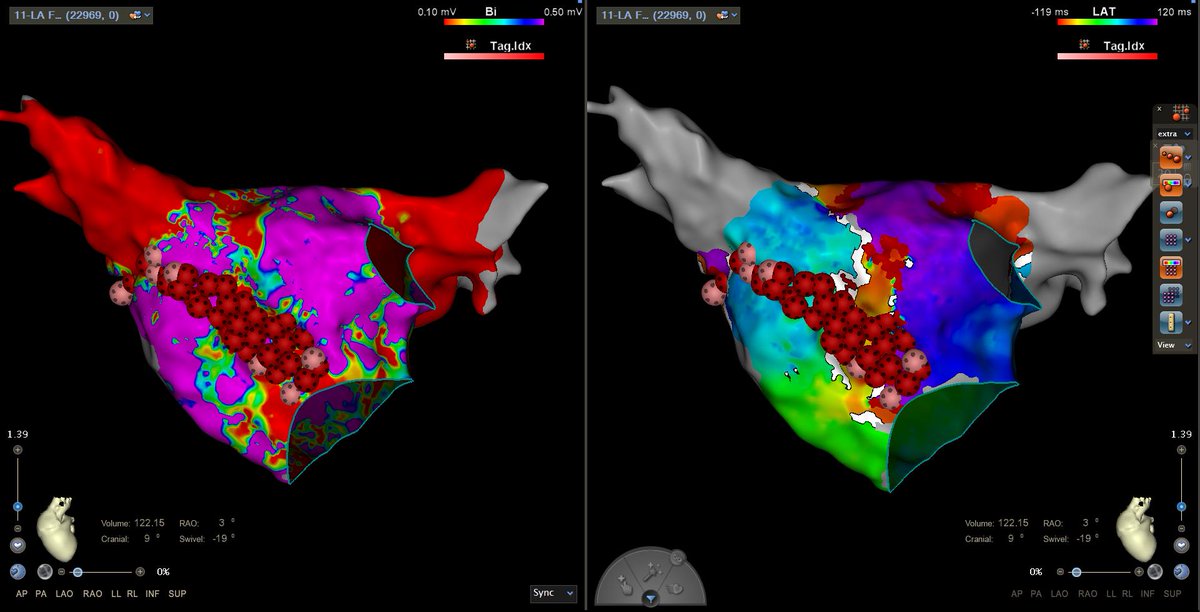
First QDOT case in CT! Patient presents three years after PVI/PWI with atrial flutter. Prior lesion set durable. Bipolar and Coherent map shows de novo flutter on the anterior septum. #EPeeps @BiosenseWebster
@MSharifpourMD Femoral stick in a morbidly obese thigh. Slide the catheter once you have a flash then you can advance your J wire. Sometimes the standard cook is too short.
@rdebiasi3@mattaustein@SergioPinski@drimdadahmed@skarim01@MDT_Cardiac That wild. I'd be interested in what the contrast shots looked like. How did you gooseneck the catheter for deployment? I assume forward pressure would push that posterior unless you added some torque at the same time.
@drimdadahmed RIPV isolation looks a little tight around the vein. Would extend that out which practically would mean eliminating that peninsula of normal voltage on the PW. Probably stop there with no triggers on isuprel.
@MarkMarieb Dual nodes with unrelated disease in the RB? You would have to assume there is a 2 for 1 response to the last stim with 2 echos to follow. That would account for the very short VA time on the last 3 beats.
@drimdadahmed@narrowQRS@Nishaki1@abhishek_mbbs@skarim01 Should be ablatable from the mid-inferoseptum. Certainly needs a revision as well. CXR would be helpful to determine wether simply moving the lead is warranted vs changing the vector with SVC or array.
@hockeypharmd Impossible to know based on what’s been released. What counts for EBM these days has progressed from peer reviewed to pre-prints, now to just press releases and surreptitiously recorded meetings. Will need to wait a little longer.
@AndrewMcGavigan EF has dropped since implant from 40s to 30s hence the original attempt was for a BLOCKHF indication. CS lead is definitely first option but first attemp was from an implanter I highly respect so planning for contingencies.
Any advice for HBP implant in a patient with persAF, currently single chamber system without an underlying? Is pacemapping for his capture an option, or maybe LBP pacemap for W in V1? Another doc failed with a CS lead but I'm going to try that first. #epeeps
@StevenZweibel@PPA_USA@doctorwes@ABIMFoundation It's also a strawman argument for MOC. Most agree there is value in initial board certification, which these studies support. Were are the studies that show MOC in its current, expensive form improves patient outcomes?
@vish_luther Assuming no CAD and no improvement with BB/ACEi would ablate AP for possible dysynchrony induced NICM. Wouldn't target the APCs unless symptomatic.