1/Time is brain! But what time is it?
If you don’t know the time of stroke onset, are you able to deduce it from imaging?
Here’s a thread to help you date a stroke on MRI!
Excited to join an outstanding faculty for the AIUM Advanced MSK US course in July, directed by Dr. Jon Jacobson! I'll be presenting the knee US lectures, and we'd love to see you in Chicago or virtually. https://t.co/s4JnOTAxK0
#AIUMMSK
1/Do you know all the aspects of, well, ASPECTS?
Many know the anterior circulation stroke scoring system—but posterior circulation (pc) ASPECTS is often left behind
25% of infarcts are posterior circulation
Do you know pc-ASPECTS?!
Here’s how to remember pc-ASPECTS!
Tired of always speculating about MR spectroscopy?
If you've ever looked at an MR spectroscopy & thought: "I have no idea what I’m looking at!"--then this cheat sheet is for you!
Here are the 4 basic rules you need so you can understand the spectrum of basic spectroscopy!
First you need to know the peaks.
3 main peaks: Choline, Creatine, NAA
Remember the order bc a spectrum looks like mountain peaks & it is cold in the mountains. And CHOld CREATures NAp or hibernate in the mountains
Choline
Marker of membrane turnover
Remember: membranes coat or “CHOat” the cell
Choline = ChoLEAN, choline LEANS into the creatine peak, it’s right next to it
Creatine
Marker of energy, basically an internal control
Remember, everyone takes Creatine powder for energy!
Creatine is at ~3—creatine almost rhymes with 3
NAA Marker of neuronal health
N = Neuron
NAA has double As so it is at ~2!
Four rules:
1. Hunter’s angle:
—Most people know that the peaks of the spectrum should go up at you move lateral, called Hunter’s angle
—Most bad things reverse Hunter’s angle
—Ask yourself: Is my arrow pointed up to shoot into the air at the enemy (good) or is point to the ground where it will hit the dirt (bad)
2. TE & spectrum length are inversely related
—Spectroscopy follows the rule: speak softly & carry a big stick.
—Short TE = long spectrum, lots of extra peaks for glutamate/glycine, myoinsitol
—Long TE = short spectrum, mainly the basic 3 peaks
3. Each region has its own unique signature
—Each brain region has its own unique composition of compounds that might alter Hunter’s angle a bit, but not reverse it
—Need a control in contralateral normal brain so compare apples to apples
4. Lactate peak goes like a sine wave
—Lactate peak represents anerobic metabolism—sign of cells in trouble
It’s at 1.3ppm. Remember this bc 13 is an unlucky number & lactate is an unlucky sign!
—It’s like a sine wave: up at short TE (35), down at intermediate TE (144), and up again at long TE (244)
—You can use this flipping to better visualize the lactate peak
—You can remember it’s down in the middle TE bc when you’re caught in the middle, you’re down & out
Just remember these tricks & you will be spectacular at basic spectroscopy!
🫁 Registration is now open for the
HRCT Pattern System for Diffuse Lung Disease
A comprehensive online course for radiologists and pulmonologists focused on a structured, pattern-based approach to chest CT interpretation.
The course covers:
✔ Reticular patterns
✔ Nodular patterns
✔ Mosaic attenuation
✔ Ground-glass opacity
✔ Consolidation
✔ Cystic lung disease
📅 Starting Friday, 22 May
🗓 9 sessions | Every Friday
⏰ 4 PM Cairo time
💻 Online via Zoom
📲 Registration & details:
WhatsApp: +20 120 678 4555
Looking forward to welcoming colleagues interested in advancing their HRCT interpretation approach.
Lateral Elbow Instability: Ultrasound Diagnosis
A 26-year-old female rugby player suffered a direct trauma to her elbow during a tackle, presenting with lateral pain associated with a lateral pivot-shift test that was inconclusive due to the patient's antalgic muscle spasm.
An ultrasound scan revealed a complete rupture in the middle third of the radial collateral ligament, which showed increased separation between its ends during valgus stress.
Conservative treatment was chosen, consisting of platelet-rich plasma (PRP) injections under ultrasound guidance at the defect site on three separate occasions, combined with orthotics in 90° flexion and pronation.
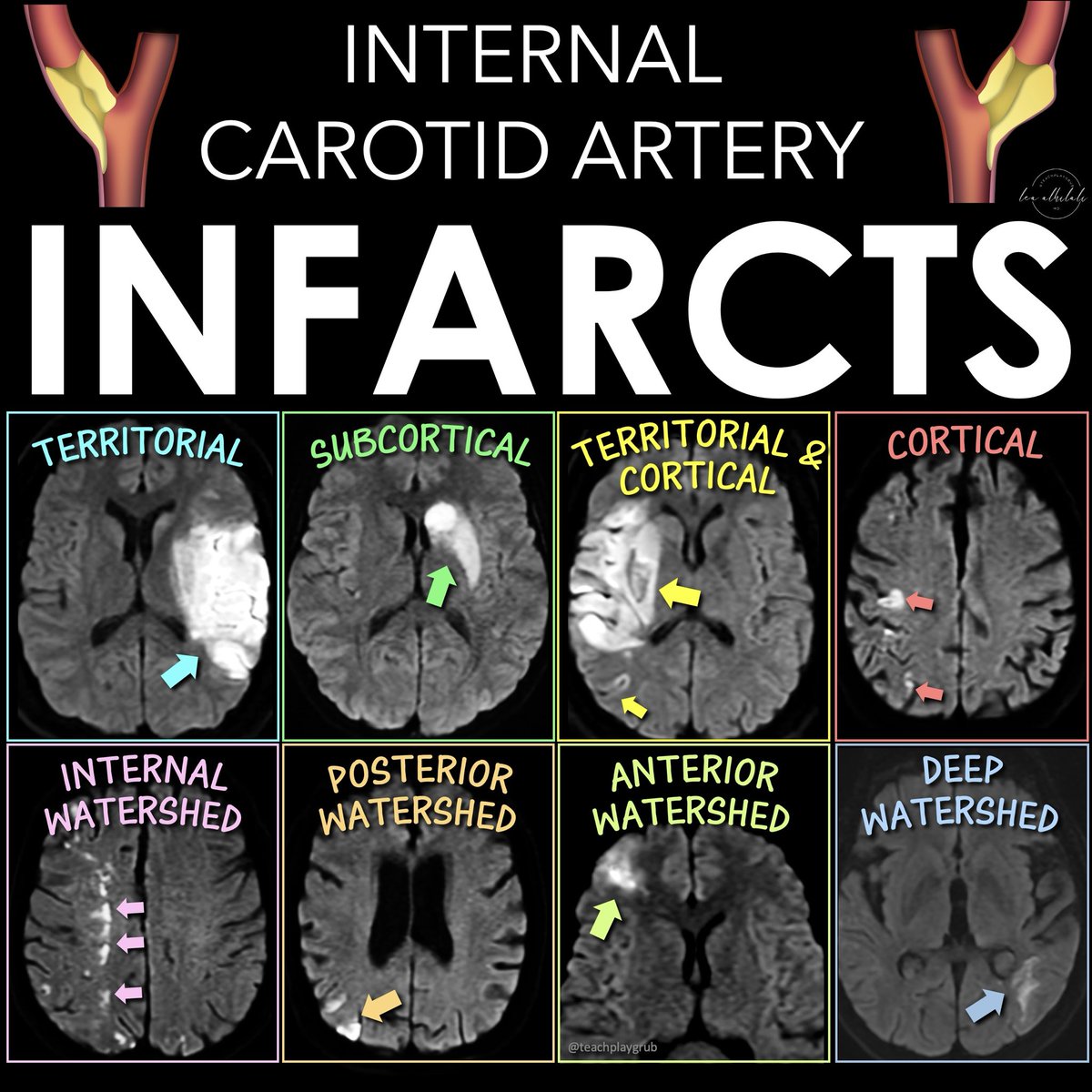
Can you get the diagnosis when it comes to carotid stenosis?
Having some confusion about the strokes you see w/ICA occlusion?
Why are there so many different patterns of infarcts w/ICA occlusion/stenosis?
There are 5 main infarct patterns—and they reflect the different types of disruption to flow you get w/carotid disease: artery to artery emboli, embolic shower, & hypoperfusion
Here’s what you see:
1. Territorial infarction w/cortical or subcortical involvement
--From artery-to-artery or distal embolism.
--More than one occlusion indicates more proximal arterial dz
2. Subcortical infarction
--When ICA, MCA, & ACA perforating deep arteries are occluded
--Can be from MCA occlusion w/good collaterals or emboli directly to deep perforating arteries
3. Combined territorial & smaller cortical and/or subcortical infarcts
--From partial embolism fragmentation or emboli shower of various sizes
4. Multiple small infarcts in the distal territories of the MCA & ACA
--If in more than one arterial territory, it’s suggestive of cardio-embolism
--If single arterial territory, it’s from a parent artery steno-occlusive lesion
5. Watershed infarctions.
Two types:
--External border-zone (located between the cortical territories of ACA, MCA, & PCA)
--Internal borderzone (between the deep & superficial networks of MCA & ACA)
--Traditionally thought from low-flow, but emboli are often a cause
--Hemodynamic mechanism may be more important in internal borderzone infarcts & embolism in external borderzone infarcts
Now you can draw the right conclusions with ICA occlusions!
Intravesical Prostatic Protrusion (IPP) is measured on ultrasound (usually transabdominal) and reflects how much the prostate projects into the bladder lumen.
Grade 1: < 5 mm → Mild
Grade 2: 5–10 mm → Moderate
Grade 3: > 10 mm → Severe
@hemo_shk MAGICAL DR Mnemonic
M - Metastasis (Most common cause of multiple ring-enhancing lesions)
A - Abscess (e.g., Pyogenic)
G - Glioblastoma
I - Infarct or Inflammatory (e.g., Neurocysticercosis, Tuberculoma)
C - Contusion (Resolving)
Common brain enhancement patterns observed on contrast-enhanced MRI, which are used to narrow down a differential diagnosis for various central nervous system (CNS) diseases.
https://t.co/FrEbwvUmgn
Can't remember the types of craniotomies off the top of your head?
Do you need another thing to memorize like you need a hole in your head?
Here's a quick figure with a review of some common craniotomies to help you out!
Let’s dig deeper into these holes!
Frontal: For large midline anterior and sometimes middle skull base lesions
Temporal: For middle cranial fossa lesions, including intra-axial lesions in the mesial temporal lobe
Parietal: For mid to posterior cerebral hemisphere lesions while sparing the motor and sensory cortices.
Parietal interhemispheric approach for parafalcine, medial parietal, and splenial lesions. Parietal transcortical route for intra-axial lesions through the functionally “silent” superior parietal lobule
Pterional (frontotemporal): Access to the frontal lobe, temporal lobe, and Sylvian fissure and allow for direct visualization of the microvasculature surrounding lesions in the suprasellar cistern