Qué importante es la optimización perioperatoria de los pacientes‼️
Seguro que conoces la Vía RICA... Sabes que hay actualización recién salida del horno❓
La puedes leer aquí 😊
👇🏼👇🏼👇🏼
https://t.co/FWNvPloi6m
O Globo: Morre Angelita Gama, médica pioneira da coloproctologia no Brasil e referência mundial no tratamento do câncer de reto, aos 94 anos https://t.co/0BtBHXNhHx
Updates on Management of Anal Cancer: A New Era Has Begun | American Society of Clinical Oncology Educational Book
🟢Free Access
https://t.co/IyPUAvzKYv
🆕 Research | Adjuvant chemoradiotherapy versus completion total mesorectal excision after local excision for early rectal cancer (TESAR): a multicentre, randomised, controlled, phase 3, non-inferiority trial
https://t.co/aBfWfRHOg6
#OncTwitter#GITwitter#rectalcancer
This is a thoughtful and optimistic overview of emerging surgical techniques for ileocolic Crohn’s disease. You do a great job framing the practical realities (surgery isn’t curative, bowel preservation is critical, and recurrence remains a major challenge) while highlighting two promising mesenteric-targeted approaches without overhyping them.
Regarding mesenteric excision, the idea that the mesentery isn’t just passive scaffolding but can act as an inflammatory reservoir makes a lot of biological sense. Extending the mesenteric resection (similar to oncologic principles) is a logical evolution, though it requires careful technique to avoid vascular or autonomic issues.
Feliz lunes a todos! Después de la resaca del #AECP2026 de Toledo, hoy
caso clínico rápido.
💁♀️ 49 años, multipara y fístula transesfinteriana anterior baja. Continencia correcta. No lesiones esfinterianas previas. Muy sintomática.
¿Qué tratamiento ofreces?
Si aún no lo has hecho, te invitamos a leer el Libro Blanco sobre Cribado Poblacional del #Cáncer#Colorrectal (CCR) en España. Promovido y coordinado por @sepdigestiva, describe la situación de programas poblacionales de cribado CCR españoles, realiza un análisis estratégico y establece recomendaciones.
Acceder desde aquí https://t.co/s9vIPVINwH
🚨 Don’t miss the prestigious @Dukes_Club Lecture #ACPGBI2026 with Prof George Chang on
🩺 “Advanced Rectal Cancer”
Chaired by@ioannadrami (Dukes’ Club President)
A key session for anyone involved in colorectal surgery & oncology
🎟️ Register now: https://t.co/6mgocqB7S8
Tomorrow. Dr @AnaOtero_MD demonstrates robotic LAR and mesorectal dissection. The session covers systematic landmarks from docking to ICG perfusion assessment. Educational video available May 20. https://t.co/voXRLb0nnd #Surgery#MedEd
Join us for a FREE TCOL virtual session! Sign up here --> https://t.co/RwxZeGsFUs
On 9 June our EIC Dr Perez and AE Dr McKechnie will host coauthors Dr Meyer and Dr Douissard for the presentation and discussion of their TCOL article "Fascial closure techniques at stoma reversal"
Practice Pearls this month with a clarification of the concepts of total and tailored mesorectal excision for rectal cancer by Drs Moran, Laurberg & Heald. Read more in this month's #DCRJournal: https://t.co/sMhvTXmavE
Joint ESTRO - ESR talk on rectal cancer. My take-away: Anatomy remains core for treatment selection. However focus should also be on predicted biology, response, preservation of function and quality of life. @GI_RadOnc@OncoAlert#ESTRO26@estro
Response to the Letter to the Editor "Organ Preservation in Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy With Endoscopic Submucosal Dissection" Read the authors' response now in #DCRJournal: https://t.co/hJbD0gwI9H
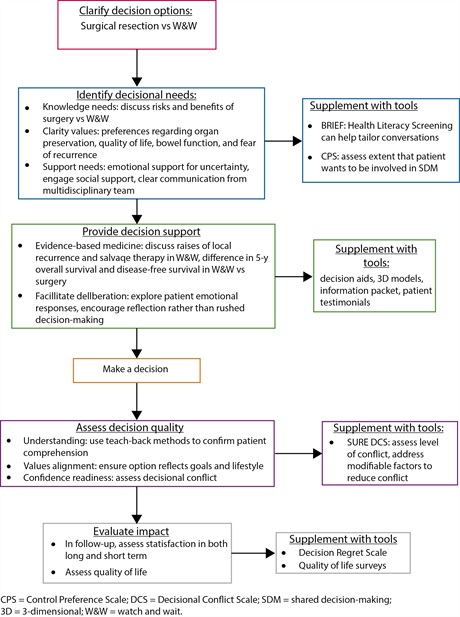
This is a great read on watch & wait in rectal cancer.
B/c patients with local regrowth after WW have higher rates of distant mets, there has been an intuitive fear that regrowth is causal (i.e delaying TME permits metastatic seeding hence WW risky).
The authors here argue (and I agree) that regrowth/metastases are manifestations of intrinsic aggressive tumor biology because:
1) no difference in time to surgery in patients w pCR/regrowth who developed mets vs. those who didn't (if delay were causal, would expect longer delay in patients who developed M1).
2) in OPRA secondary analysis, patients with cCR underwent least surgery/longest observation while those with incomplete response had surgery most frequently/immediately. But outcomes still tracked with response phenotype not timing of surgery (i.e. cCR did best).
3) tumor response itself is prognostic (i.e. even when all pts undergo TME, more regression after neoadjuvant therapy --> better DFS/DM).
4) modern tumor evolution data suggest metastatic spread mostly happens early.
5) chemo/radioresistance appears to be linked to metastatic potential (i.e. regrowth is a marker of aggressive biology not the mechanism itself).
IMO a persuasive argument against hypothesis that regrowth seeds metastasis, but rather biology=dominant driver. @OncoAlert