Ventricular free-wall rupture, ventricular pseudoaneurysm, and papillary muscle rupture complicating acute myocardial infarction: A clinical consensus statement of the ESC Working Group on Cardiovascular Surgery... Read more in the @EHJ at https://t.co/Aj1fXdgQsT #CardiovascularSurgery #AcuteMyocardialInfarction #CardioVascularCare @ESCardio@ESC_Journals
In the GLUCO-TAVI trial, 100 patients undergoing TAVI were randomized (1:1) to peri-procedural glucocorticoids (IV methylprednisolone + 5-day oral prednisone) vs standard care to evaluate whether inflammation modulation could reduce post-TAVI conduction disturbances requiring pacemaker implantation.
At 1 month, permanent pacemaker implantation occurred in 8% of patients receiving glucocorticoids vs 16% in the control group (RR 0.50, 95% CI 0.16–1.55; p=0.23), showing a numerically lower event rate, although the study was not powered to demonstrate statistical significance.
At 1 year, no significant differences were observed in PPI (RR 0.67; p=0.41) or new LBBB (RR 1.12; p=0.66).
Peri-procedural glucocorticoid therapy was feasible and appeared safe, with no signal for excess complications, mortality, or adverse events.
These hypothesis-generating findings suggest that a short course of glucocorticoids represents a potential strategy to reduce post-TAVI conduction disturbances. Evaluation in larger, adequately powered randomized trials is warranted before any conclusions regarding clinical applicability can be drawn.
ARTICLE: https://t.co/ATRb0ICWWH
EDITORIAL: https://t.co/subFyAQN9z
🫀🔥 When myocarditis is not just myocarditis…
A new study by sheds light on a critical and often under-recognised entity: desmosomal “hot-phase” cardiomyopathy (HPC).
💡 Why does this matter?
Because HPC can mimic acute myocarditis, but carries a much higher arrhythmic risk and different clinical implications.
🔍 Key insights from the study:
👉 Patients with desmosomal HPC are often:
• 👩⚕️ Young and female
• 🧬 Carriers of desmosomal gene variants (mostly DSP)
👉 Compared to classic myocarditis, HPC shows distinctive “red flags”:
🧾 Clinical clues
• Family history of cardiomyopathy / sudden cardiac death
• Recurrent troponin elevations (“hot-phase” relapses)
🧲 Imaging clues (CMR)
• Ring-like late gadolinium enhancement (LGE)
• Right ventricular involvement
• Persistent or progressive LGE
• Incomplete recovery of LV function
⚡ Electrical clues
• Low QRS voltages
• High arrhythmic burden
• Ventricular arrhythmias at a young age (<45 yrs)
📊 A practical takeaway
A simple combination of:
➡️ Ring-like LGE
➡️ RV involvement
➡️ Family history
🎯 Achieved ~93% diagnostic accuracy in identifying HPC.
🚨 Clinical implication
Recognising these red flags early can:
✔️ Prompt genetic testing
✔️ Improve risk stratification
✔️ Prevent life-threatening arrhythmias and adverse outcomes
💭 Bottom line:
Not all myocarditis is inflammatory.
Some cases are the first manifestation of a genetic cardiomyopathy.
👉 We need to think beyond the diagnosis and look for the phenotype.
#Cardiology #Cardiomyopathy #Myocarditis #CMR #CardiacMRI #Arrhythmia #Genetics #PrecisionMedicine #DSP #ACM #HeartDisease #MedicalResearch #CardioTwitter
https://t.co/0CW1Hkl7nS
#EHJCVI 🔍 Integrating CT, CMR, and PET-CT is critical for correctly distinguishing structural vs non-structural prosthetic valve dysfunction, detecting thrombosis or endocarditis, and guiding reintervention before clinical deterioration. Read more 👉 https://t.co/FzkRLJunuD
Check out our new contemporary review on multimodal imaging for heart transplant surveillance, now published in JAHA. #EchoFirst#ThinkPET#YesCCT#CMR
https://t.co/t3WaPqQKBt
A new paper in #EHJ redefines endotypes of angina with non-obstructive coronary arteries. Read the results of prospective multicentre study 👉 https://t.co/8soSNZkPXb
@RoccoMontone@ehj_ed
Bad news for enthusiasts of left atrial appendage closure from #AHA25. CLOSURE-AF is not yet published, but reports from New Orleans indicate inferiority compared with best medical care (the trial was designed for non-inferiority, making this the most unexpected and unfavorable scenario).
In 888 patients with atrial fibrillation considered at high risk for stroke and bleeding, a composite endpoint of stroke, systemic embolism, cardiovascular or unexplained death, and major bleeding occurred in 16.83% of patients who underwent left atrial appendage closure and 13.27% of those receiving best medical care (whose exact definition remains unclear — we’ll hopefully find out once the paper is available).
These appear to be patients in whom the appendage is perhaps closed somewhat lightly — the rationale often being “so they won’t need lifelong anticoagulation.” Well, lifelong benefit remains to be seen, but after a median follow-up of 3 years, the risk of events was 28% higher with appendage closure, with a 95% confidence interval for the hazard ratio indicating a potential 1 to 62% increase in risk.
In short, the results are not definitely encouraging, and much remains to be understood. Which events increased? Likely ischemic ones. And further — was it appropriate for the trial to combine ischemic and bleeding events, along with cardiovascular death, into a single non-inferiority endpoint? Probably not, yet the findings have disrupted expectations and made the discussion quite compelling nonetheless.
Finally, could the expected long-term reduction in events (beyond 3 years, potentially lifelong) eventually offset the initial, possibly procedural and hemorrhagic, risks — shifting the balance back in favor of closure for patients with longer life expectancy and prolonged exposure to anticoagulation? Hard to say without full data. And in any case, this is only one trial; at least three others are ongoing in high bleeding-risk populations (STROKECLOSE, CLEARANCE, and LAA-KIDNEY).
Let’s also recall that somewhat more favorable data have been seen in anticoagulation-eligible populations, but at this stage it seems appropriate to pause and reflect.
If you’d like to reflect with us, join the @escardio webinar on Monday, where I’ll also be participating — it feels perfectly timed.
https://t.co/7KSEXSBODA
Inflammasome and ventricular arrhythmogenesis: Pathogenic interplay and potential targets on the horizon
Learn more on Trends Cardiovasc Med. 2025 Jun 11:S1050-1738(25)00077-5. doi: 10.1016/j.tcm.2025.05.006. Epub ahead of print. PMID: 40513627.
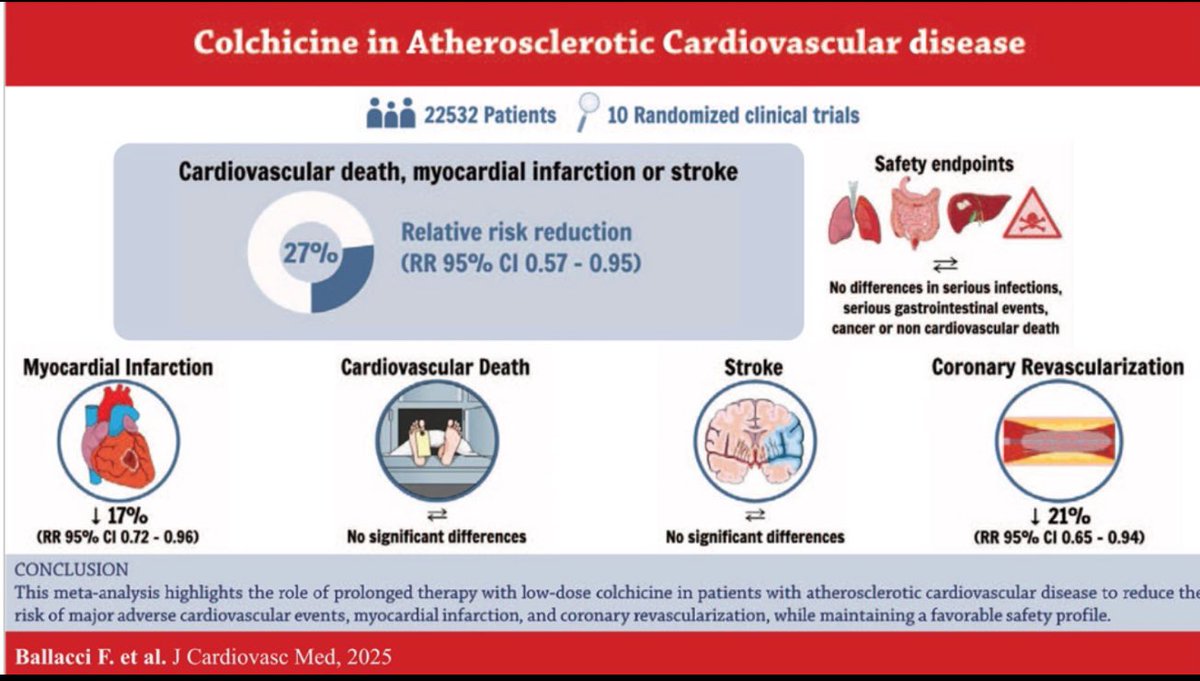
Colchicine for prevention of major adverse cardiovascular events: myth or reality?
Lear more on J Cardiovasc Med (Hagerstown). 2025 Jun 6. doi: 10.2459/JCM.0000000000001744. Epub ahead of print. PMID: 40530569.
New Clinical Consensus on Left Atrium & Left Atrial Appendage Imaging 🚨
The #EACVI with EHRA has released updated guidance on #MMI for the assessment of the Left Atrium (LA) & Left Atrial Appendage (LAA).
This evidence-based document is essential for improving diagnosis, management, and prognosis of conditions like #AF #HF & cardioembolism. A must-read for all cardiologists and #CVImaging specialists!
Read the full consensus https://t.co/ylNDBlEyOZ
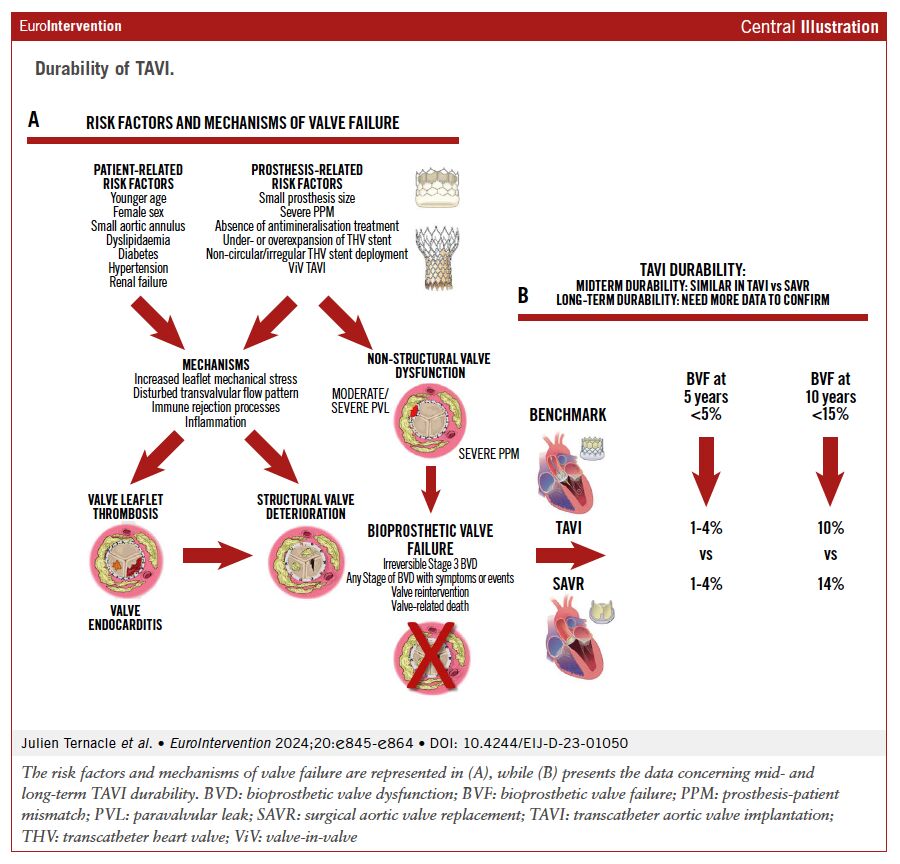
This comprehensive review examined the durability of TAVI compared to SAVR, addressing definitions, mechanisms, and long-term data on bioprosthetic valve dysfunction and failure. While midterm outcomes are comparable, long-term durability remains to be fully established. @TernacleJ @PPibarot
https://t.co/6YSyYKriZq #Cardiology #MedicalResearch #TAVI #SAVR #HealthcareInnovation
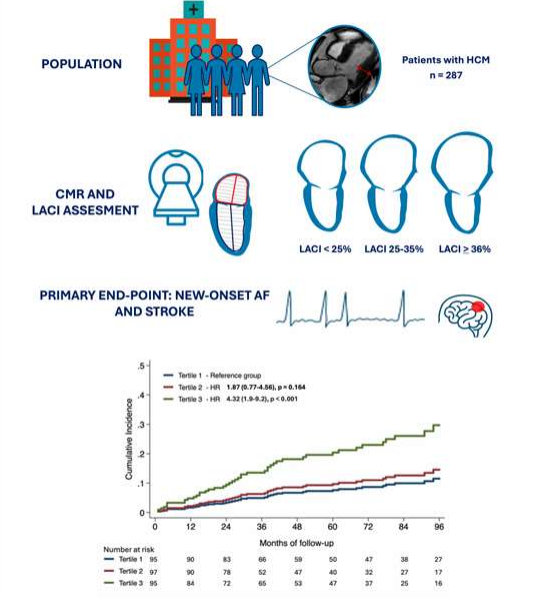
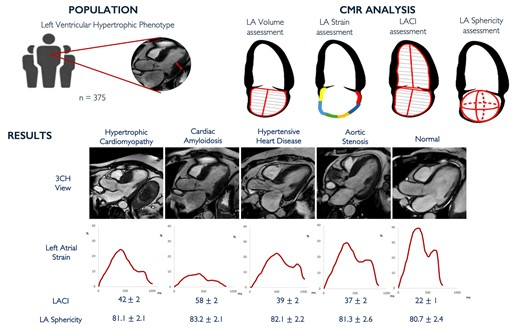
How does the left atrium remodels in the various etiologies of LV hypertrophy? @MartinaRaffele provides you more information about it 👇👇👇https://t.co/KSAyYC5o6J
Kudos to Martina and the Cardiovascular Imaging team of the @IcorCat @GermanECediel! @hgermanstrias@GTRecerca