We've written to the Secretary of State and NHS England CEO calling for urgent action to address unsafe doctor substitution by employers.
The letter comes in the wake of our survey report revealing doctors' serious concerns over patient safety. 🔗 https://t.co/tqhjxqUQU6
Four in 10 NHS organisations are using nurses or other non-medical staff to cover doctors’ rotas because of workforce shortages, a freedom of information investigation has revealed
https://t.co/i6dX6Upl9Y
"I think it is scandalous that the NHS is allowing the substitution of doctors by individuals without sufficient medical knowledge instead of the obvious response to doctor shortages: hiring more doctors." Dr Mel Ryan, BMA lead on preventing doctor substitution.
Advanced practitioners are being used to cover doctor rota gaps across the NHS. Read more: https://t.co/bwksW1sIqB
🚨 Almost HALF of all NHS Trusts are using non-doctors to fill doctor rotas due to “shortage of doctors”
FYI - 40,000 doctors applied for only 10,000 available training posts last year
Doctors are unemployed
Doctor substitution is real
And it’s DELIBERATE
As the latest round of unnecessary strikes come to an end, I have written to the BMA Resident Doctors Committee asking to meet the whole committee.
It’s time for the BMA to be realistic and reasonable about what the country and the NHS can afford.
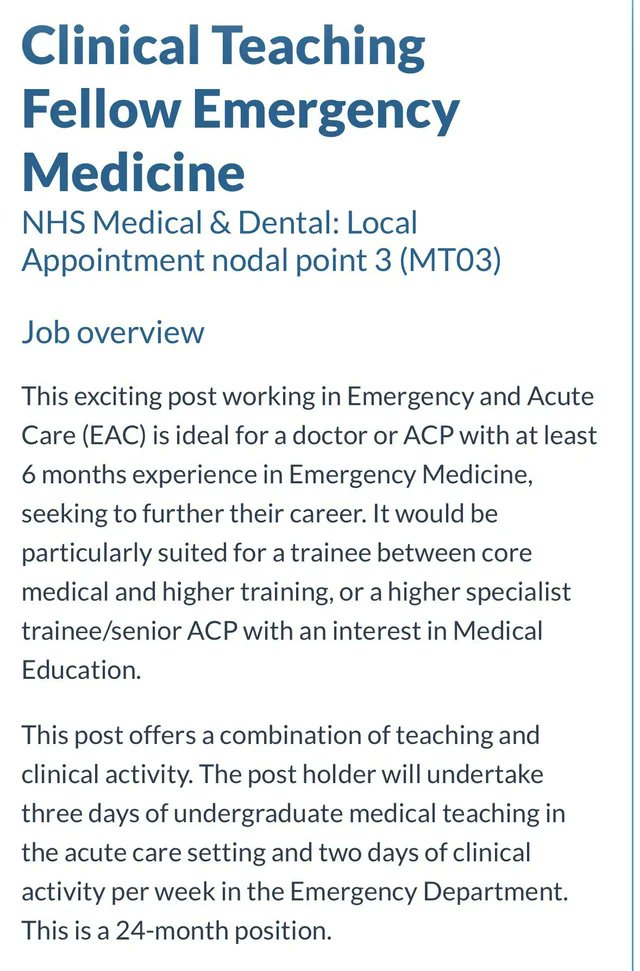
Hello @nottmhospitals
I’m happy to arrange a teaching session for your recruitment lead to reiterate that ACPs (physios, podiatrists, pharmacists, etc.) are not equivalent to EM registrars.
They must not be allowed near this vacancy.
ACPs are unqualified for this role.
@ExplosiveEnema2 Thanks but no Thanks!
Striked everytime since I arrived in the UK, just for you guys, I never cared about these strikes But i striked so you guys can have a good pay as you need to support your family
But Naaaaaaaah!
I am back stabbed by the BMA RDC! Will leave happily if needed!
Got a Rank of 204/3800.
Worked for roughly 2 years in the NHS.
And I am not in priority group because someone whose rank is 3800 will get the offer because of their Passport or ILR status.
Literally Heart Broken !
I’m keeping my promise to resident doctors.
We’re looking after our homegrown talent.
Thanks to @fletchjack and @BMAResidents for working together with us on this.
@DrInsurgent Every country in the world chooses a more Competent person, otherwise they are bound to Fail
Thats how you maintain providing top healthcare!
USA doesnt prioritize americans by law, if you score 270 and an American scores 250, you will get training. Anyways, best of luck to you !
We are exploring the use of advanced practice roles by NHS employers. To help inform our work, please complete our survey, which is open to all UK doctors and medical students.
https://t.co/Hoy2wYj4ER
@fletchjack Been working in A & E for 2 years now, got IMT interview and applied for ED msra on 19th, but wont be giving it now
We supported you in Strikes, We voted everytime because of you and in return
You guys have thrown doctors like me under the bus
Will cancel my membership today
I translated this into English for everyone to read. This is written by an orthopedic surgeon colleague in Spain, but I know my American colleagues will appreciate the text an similarities to challenges we face here
1/
The Asymmetry in Medicine in Spain: Responsibility Without Authority (I)
Opinion
Francisco J. Guitián Lema
The Asymmetry in Medicine in Spain: Responsibility Without Authority (I)
“There is irrefutable empirical proof of this asymmetry: the doctor can replace anyone; no one can replace the doctor,” states Francisco J. Guitián Lema, a Vigo-based traumatologist specializing in orthopedic surgery
There is a truth so elementary that it feels uncomfortable to state it: a hospital exists solely and exclusively to cure the sick. It is not there to provide jobs or to justify organizational charts. Nor to feed bureaucracies or to experiment with organizational theories. It exists so that a sick human being leaves it less sick or, at the very least, having received the best possible treatment.
From this premise follows a logical consequence that the Spanish healthcare system seems determined to ignore: in that healing process, there are only two absolutely indispensable figures. The patient, who is the reason for the entire structure’s existence, and the doctor, who possesses the knowledge to guide that process. Everything else — and this is not disdain, but taxonomy — is support structure. Necessary, valuable, often heroic, but auxiliary.
The doctor is the only professional capable of performing the core act that justifies the hospital’s existence: diagnosing the disease and establishing the treatment. Without a diagnosis, there is no possible direction. Without a therapeutic indication, there is no meaningful action. An orderly transports the patient, but it is the doctor who determines where and why. A nurse administers medication, but it is the doctor who decides which, how much, and when. A technician performs a test, but it is the doctor who orders it and interprets its result.
This functional hierarchy is not a social convention or an inherited privilege: it is a direct consequence of training. Six years of medical school plus four or five years of MIR specialization produce a professional capable of integrating knowledge of anatomy, physiology, pathology, pharmacology, and a thousand other disciplines into a diagnostic synthesis that no other healthcare professional is trained to perform.
There is irrefutable empirical proof of this asymmetry: interchangeability. A doctor can, in case of need, perform the functions of any other hospital professional. They can push a stretcher, insert an IV line, draw blood, take vital signs — in Germany, doctors routinely perform these functions. The reverse is not true. An orderly cannot diagnose pneumonia. A nurse cannot order a surgical intervention. The doctor can replace anyone; no one can replace the doctor.
Recognizing this reality does not imply disdain toward anyone. Nursing care is essential. The orderly’s work ensures that hospital flow does not stop. Everyone deserves respect and fair compensation.
But respect for personal dignity cannot be confused with functional equivalence. In an operating room, the surgeon is not worth more as a human being than the assistant; but their function is irreplaceable in a way that the assistant’s is not.
This distinction, obvious in any other field, has become taboo in Spanish healthcare. The prevailing egalitarianism has managed to make an evident functional truth be perceived as a moral offense.
While it is hard to pin blame on a single action, the Nottingham UTC should have recognised the seriousness. Yet again we see a unit staffed by noctors: ACPs and PAs, with no actual doctor present. It is unacceptable, and a patient has paid the price.https://t.co/zdL3r07W4Z
The UK @ternfellow EDcorridor study is out!
Key points
1. 1in5 are treated in ED escalation areas (eg corridors)
2. 10-25% of EDs have no available resus cubicle
3. The problem/solution is flow. More patients waiting for beds in ED than in corridors.
https://t.co/r5wna1PDMP
It was greedy doctors in the past, didn’t get enough coverage? Now Blame it on the poor sick patients who either
1. Can’t get GP appointments (No jobs for them from Govt)
2. Or wait in ED for multiple hours to see a doctor mostly on uncomfortable chairs or in corridors
ridiculous