MD focused 24/7 on Wt. mngmnt since 2004. Director Medcan Wt. Mngmnt, Director Mt Sinai Hospital High Risk Pregnancy Wt. Mngmnt. Lecturer University of Toronto
Me: At conference eating a sandwich. Keto guru Doc: “You know that bread will kill you”. Me: “My grandfather lived to 104 years old”. Keto guru Doc: “By eating bread”? Me: “No, by minding his own business”.
The GLP-1 receptor agonist semaglutide (Ozempic®/Wegovy®) -soon to be available at 7.2 mg once weekly- has been shown to reduce the incidence of cardiovascular death, non-fatal heart attacks, and non-fatal strokes in people living with established heart disease and overweight or obesity.
So… cardiologists will now be prescribing GLP-1 agonists to their patients more frequently.
If you are someone prescribing a GLP-1 receptor agonist or personally starting one, you’ll find this podcast extremely relevant.
I was recently invited by @Dr. Grace Chua and the @Canadian Cardiovascular Society to discuss exactly this on the Cardio Connector Podcast episode “Sustaining Success: Real-World Approaches to Obesity Management.”
In the episode, I share three key principles every cardiologist should integrate when prescribing these medications:
1️⃣ Addressing internalized weight bias 2️⃣ Discussing appetite dysregulation 3️⃣ Setting realistic weight loss expectations
Integrating these principles is:
🔹 Straightforward ✅ Simple ⏱️ Not time-consuming ⚡ Yet critical
I suggest that doing so will meaningfully improve:
✅ Medication adherence ❤️ Clinical outcomes
🎧 Listen to the full episode here:
https://t.co/aJF7ZDpTK1
What challenges or successes are you seeing when discussing GLP-1 therapies with your patients (or in your own experience)? I’d love to hear your thoughts in the comments 👇
#Cardiology #GLP1 #Semaglutide #Ozempic #Wegovy #ObesityMedicine #PatientAdherence #CanadianCardiovascularSociety #HeartHealth
@shaunmmaguire@sethbannon@msuster@grok Obesity medicine expert here. FYI fMRI is validated and provides our best in human mechanistic data showing how people with obesity have hyper responsivity to food stimuli (photos) in the “human motivation to food system”.
@drmarkhyman Insulin resistance does not cause obesity. Obesity causes insulin resistance . Over eating does not cause obesity. Obesity causes over eating.
@KevinH_PhD@AaronHengist Hey Kevin, why are you and now @AaronHengist testing the effects on sleeping energy expenditure of nicotinamide ribosome supplementation?
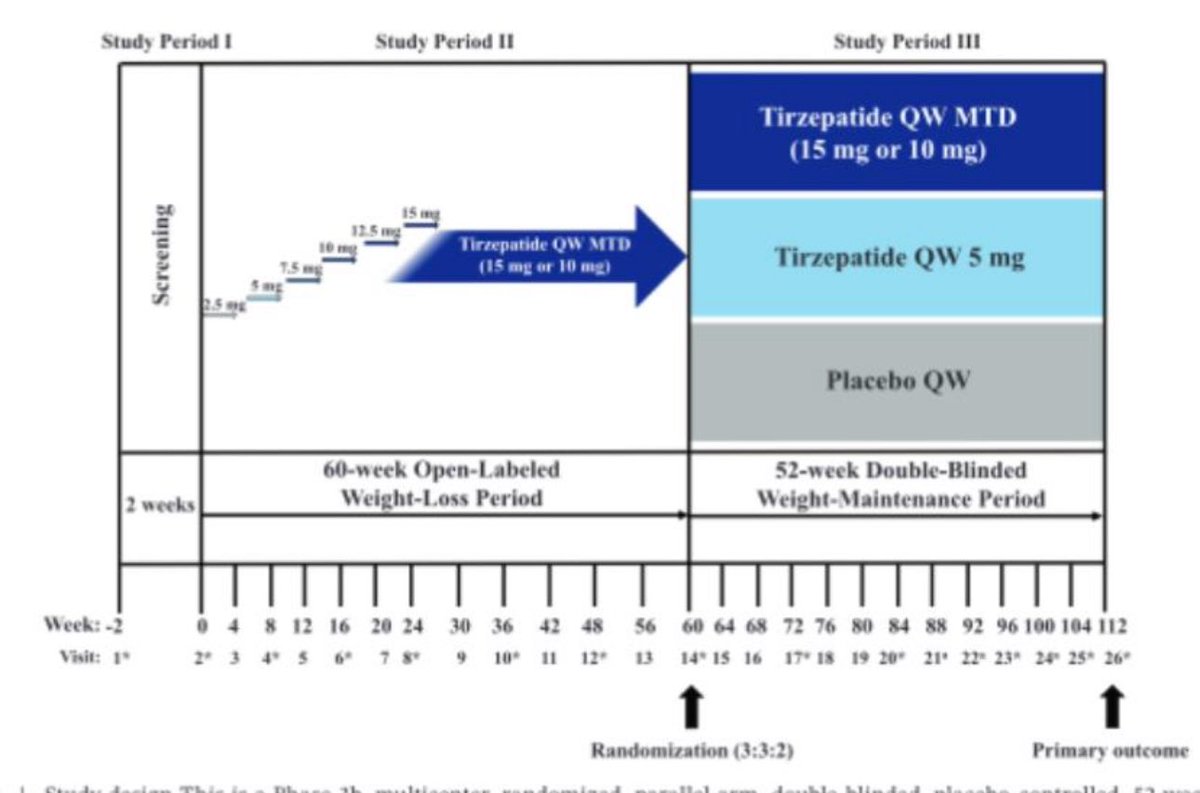
Standing room only in Malaga Spain at #ECO2025 as Dr. Horn presents the landmark Surmount-5 trial data published today in NEJM. https://t.co/nNsMMQRzUq
@MichaelAlbertMD @GLP1Insider Hey Michael, I am at ECO in Malaga Spain this week. I’m sure this will be a hot subject, I’ll be sure to mention your data.😀Congratulations, yours is a model obesity clinic👍
@sguyenet@HermanPontzer Hey @sguyenet and @HermanPontzer, happy new year. Quick switch to the other side of the energy equation. High levels of exercise leading to lower calorie intake as a consequence of ⬇️ incentive motivation and ⬆️ executive self regulation? Lots of evidence there…
@Tellit007@MichaelMindrum Thinking this through… Why are obesity rates in Kuwait, Qatar, and Egypt equal to or higher than the U.S., despite significantly lower consumption of ultra-processed foods and less sedentary lifestyles?
@Tellit007@MichaelMindrum Countries with obesity rates within 2–3% of the US often lack the same obesogenic ultra-processed food environment. What else might be driving the numbers?
@MichaelMindrum People would be tempted to say the signal is the US food environment, but the answer is likely genetics… look at the comparators. For example, US rates are similar to Kuwait. US is a melting pot of obesity associated genes.