Confession: I LOVE hyponatremia 🤓
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
Fluid overload occurs frequently in critically ill patients with AKI and is one of the indications for continuous kidney replacement therapy (CKRT). In this article, the authors state that available and emerging tools help predict and monitor volume status more actively and dynamically to best design UF strategies that avoid hypotension but alleviate congestion. https://t.co/pyqCAMGAG2
@GonzaRGuerrero
KIDNEYcon Registration is Open!
April 6-8, 2024
Little Rock, AR
https://t.co/WR0UUcbmUN
Little Rock will experience the 2024 Total Solar Eclipse
Discount room rates at the DoubleTree Hotel!
@NephroRock@nephrosharma@nephrosingh@VelezNephHepato@kidney_boy
Re-reading excellent thread by
@NephroMD. In Winzeler paper, UOsm>=500 is highly specific for non-responsiveness but v. insensitive
🤔How about:
UOsm>500: don't bother with FR
UOsm<300: FR should be first-line approach
300-500: Consider trial of FR
❓
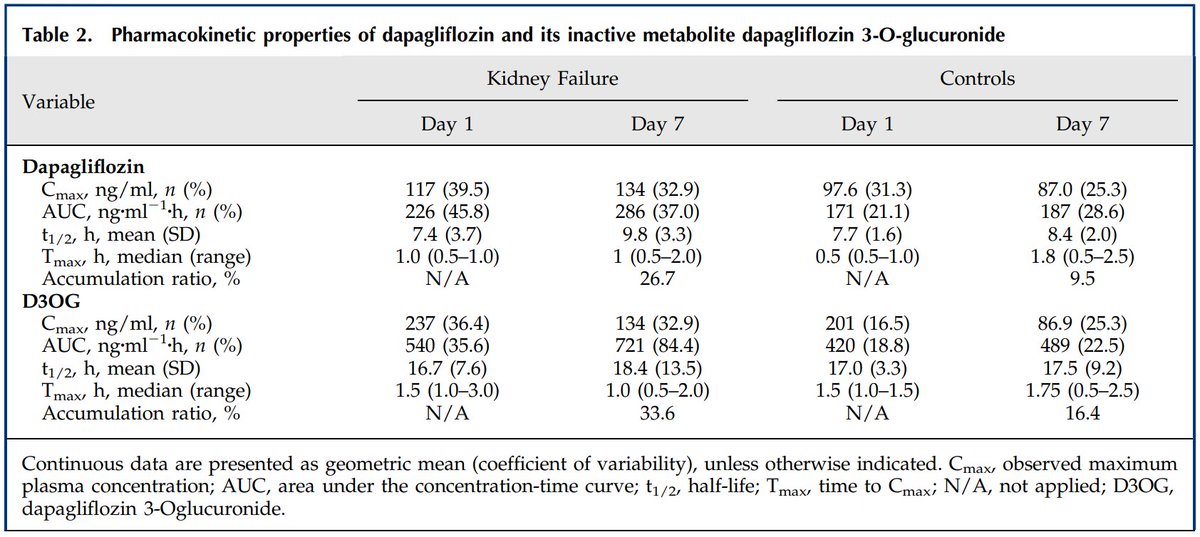
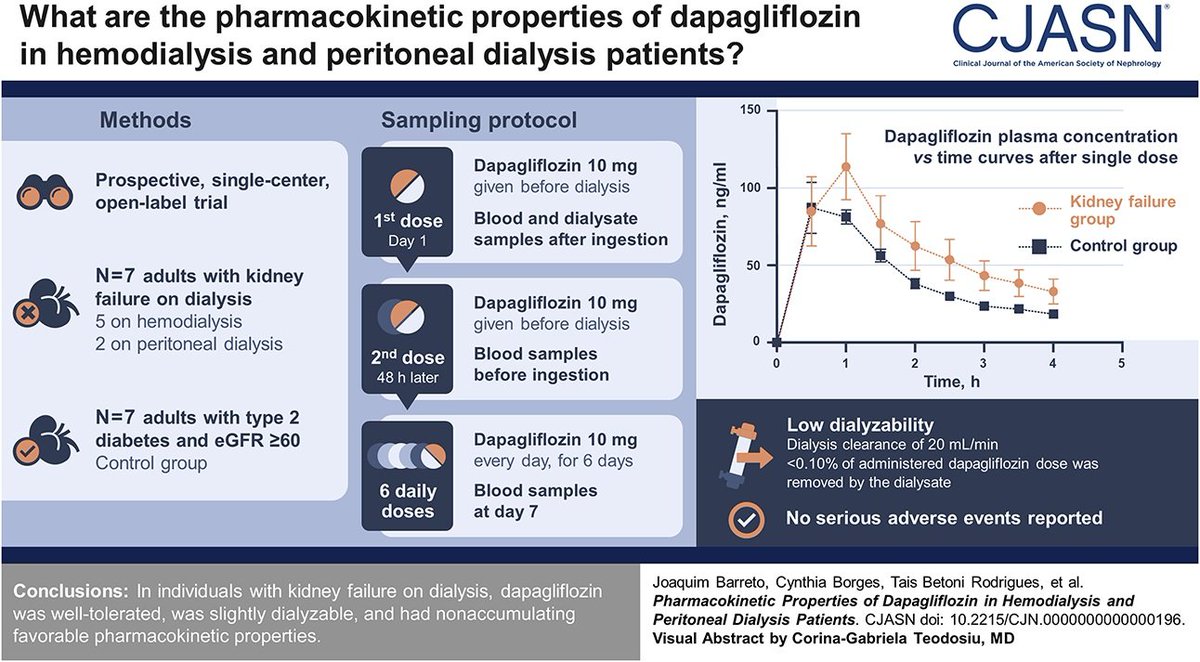
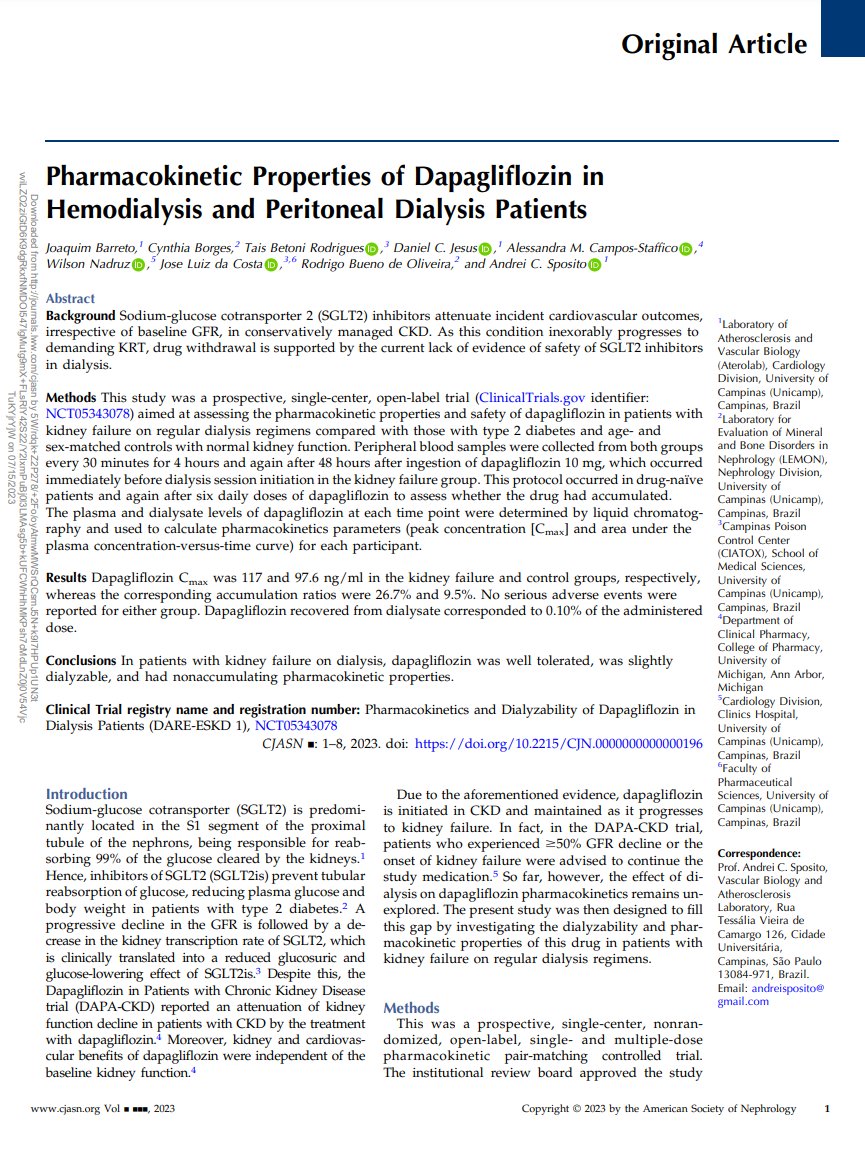
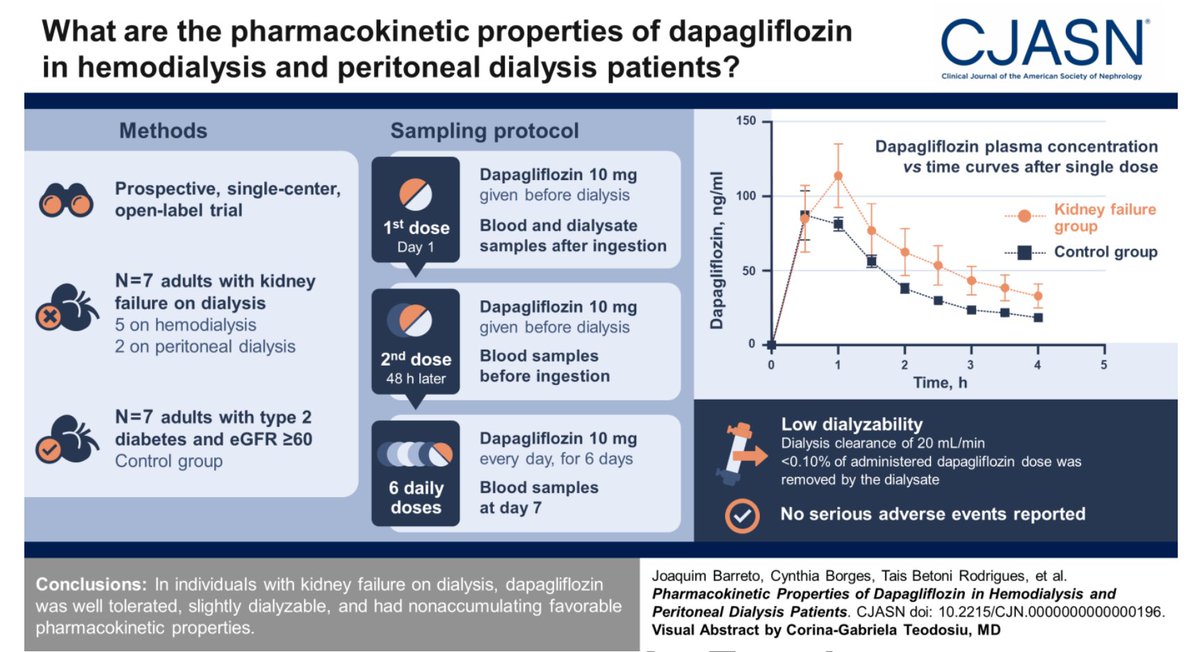
DARE-ESKD 1: Pharmacokinetic Properties of SGLT2 inhibitor (SGLT2i) Dapagliflozin in Patients on Hemodialysis and Peritoneal Dialysis ca. 2023 from @CJASN #Nephpearls
- Well tolerated
- Slightly dialyzable
- Non-accumulating pharmacokinetic properties
https://t.co/cTRliEUxPG
Looks like you can #Flozinate your dialysis patients!
"In individuals with kidney failure on dialysis, dapagliflozin was well-tolerated, slightly dialyzable, and had non-accumulating pharmacokinetic properties"
https://t.co/EUs4jsFEop
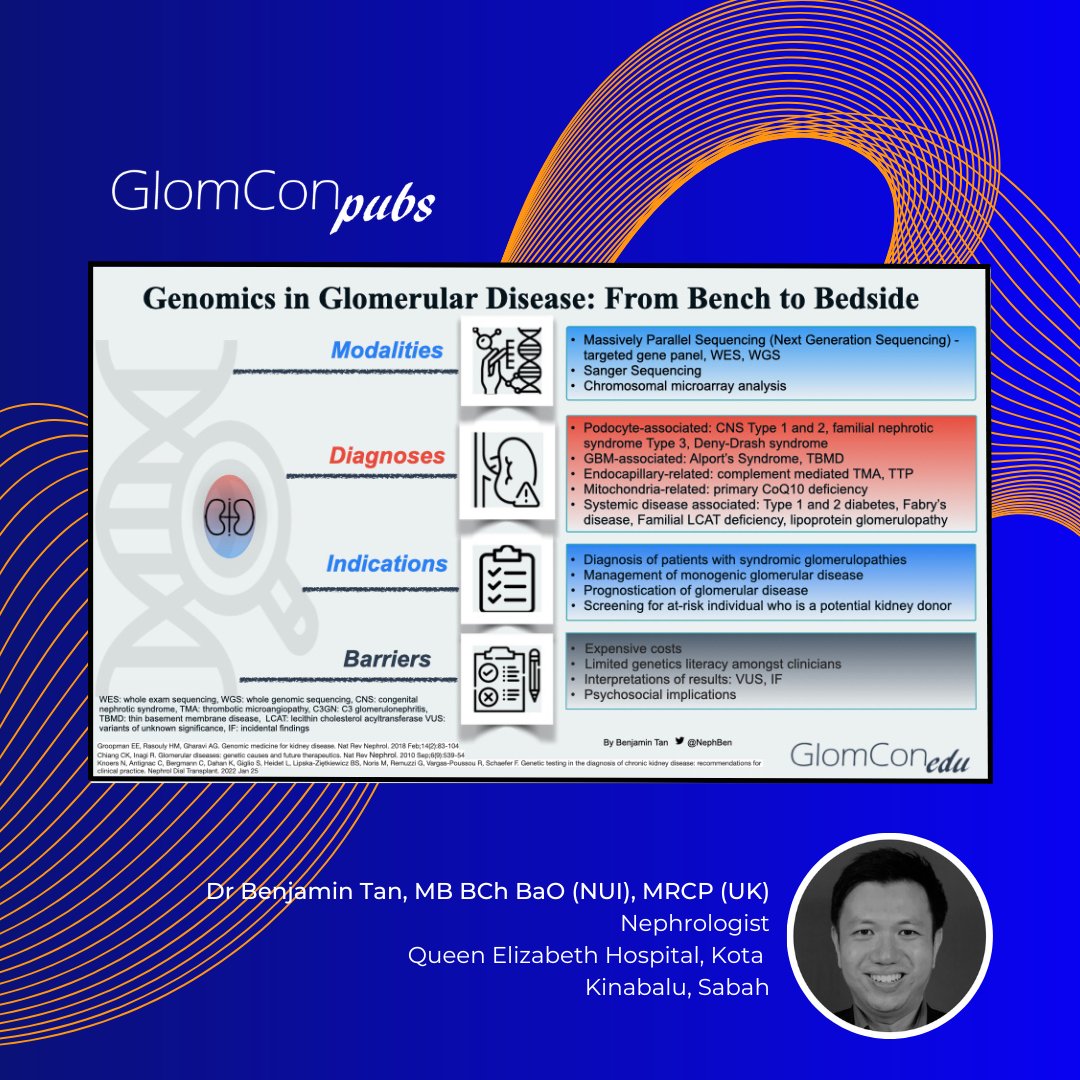
Genomics in Glomerular Disease
A GlomCon Pubs summary on genetic diagnoses of glomerular diseases by Dr. Benjamin Tan @NephBen
Read more 👉🏻 https://t.co/HCnimnzIdv
#GlomCon
Our article in @NatRevImmunol proposes that nephritis can be classified primarily according to cause, then by the lesion. This would improve management, education, understanding and research.
Thanks to @hjanders_hans@PRomagnani and Prof Nelson Leung for a great collaboration.
Ambulatory Hemodialysis Unit Rounds:
Called to see a patient with hypotension: BP 76/40,🧠 OK, CRT 5 seconds
1st step ➡️🛑Ultrafiltration + 300 ml bolus. BP 90/60
Pt is a middle aged ♂️ w ESRD and T2DM
1/9 🧵
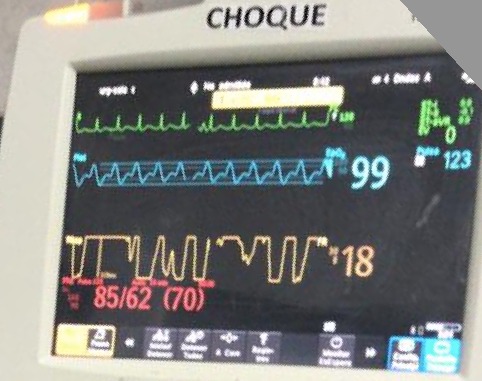
#AKIConsultSeries:👨w T2DM➡️🏥 for fever, dysuria and CVA tenderness. On arrival: ⬇️BP, ⬆️Glucose, ⬆️AGMA. Dx UTI + DKA. Tx: Abx + Insulin Pump + 4 L Crystalloid + NE
After resus, pt still oliguric, Cr 3.2. NE 0.7 ug/kg/min,🧠confused, BP 85/62, HR 123, 2L O2. CRT 4 sec
1/12