Detecting lung cancer 5 years before it happens, in @CellCellPress courtesy of the @CharlesSwanton group.
Astonishing translational work !
https://t.co/EvUmIGVLgs
We have never run a sham-controlled RCT for total knee replacement.
Not once. The most commonly performed orthopedic procedure in the United States, 700,000+ per year, has never been tested against placebo.
And yet when low-dose radiotherapy (LDRT) for knee OA is presented, the first objection is always: "Where's the sham-controlled data?"
That double standard is worth naming out loud.
Here is what LDRT actually has:
→ 2 positive sham controlled trials (Korean and Iranian)
→ A 292-patient prospective RCT (Russian) with 11 year follow-up
→ 4.5x difference in pain scores at 36 months across every domain (pain, stiffness, function, quality of life)
→ Plain-film radiography and MRI at 10 years showing a statistically significant reduction in marked progression
→ A 50-year European safety record with no meaningful toxicity
Here is what the treatments currently in OA guidelines have:
→ NSAIDs: known cardiovascular, renal, and GI harm at chronic doses
→ Glucosamine/chondroitin: failed large RCTs. Still in some guidelines.
→ Corticosteroid injections: emerging evidence of accelerated cartilage loss with repeat use
→ TKA: no sham trial. Ever.
If LDRT was a pill, it would be in every guideline.
The evidence bar being applied to LDRT is not being applied to anything else in this space.
The critics aren't wrong that we need a multicenter sham-controlled trial. We do. That's the ask.
But the argument that the current evidence is insufficient to justify treatment while we continue recommending interventions with weaker or more harmful evidence bases is not scientific rigor.
It is asymmetric scrutiny.
The field has been waiting decades for a non-surgical, disease-modifying treatment for OA. The data suggests we may have had it all along.
That conversation is overdue.
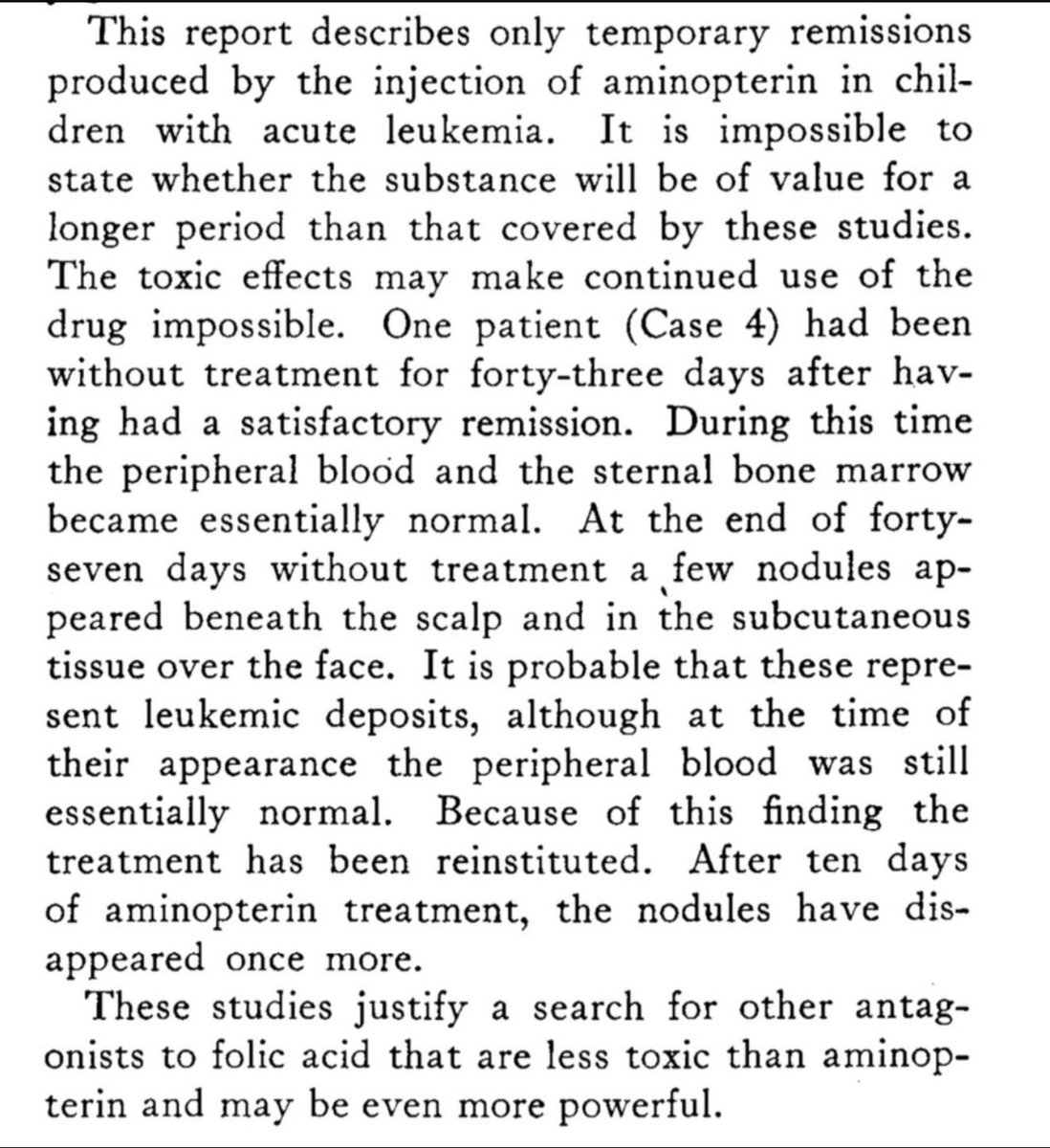
In 1948, Sidney Farber and colleagues published his work in @NEJM that helped open the door to modern chemotherapy.
Seeing that history from the same institution — especially after a remarkable #ASCO26 with major plenary contributions and @NEJM papers from @DanaFarber — is humbling.
A powerful reminder that progress in oncology is built across generations: by patients, scientists, clinicians, and teams who keep asking what might be possible.
Today, @StanfordRadOnc we treated our first patient with ultra-compact upright proton therapy. 70 years ago, Stanford also treated the first patient on the linear accelerator. #radonc
Attn Delaware - NO Listed Payments for 77387, 77402, 77407 and 77412 - @OfficialRCCSInc
Andrew Wilson
Medicaid Director Delaware Health and Social Services
State of Delaware, Department of Health and Social Services
1901 N. Dupont Highway, PO Box 906, Lewis Building
New Castle, DE 19720
[email protected]
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77387, 77402, 77407, and 77412
Dear Medicaid Director:
I am writing to you in my capacity as Chairman of R3 with clients in Delaware to express grave concern regarding the current Delaware reimbursement rates for essential radiation oncology treatment delivery and guidance services. These missing rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Delaware beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77387 (IGRT): $ NOT LISTED AS PAYABLE
· CPT 77402 (Radiation treatment, Level 1): $ NOT LISTED AS PAYABLE
· CPT 77407 (Radiation treatment, Level 2): $ NOT LISTED AS PAYABLE
· CPT 77412 (Radiation treatment, Level 3): $ NOT LISTED AS PAYABLE
Found here: https://t.co/fubrykeb9G this website: https://t.co/lWwW8GI08F
This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care. By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77387 (pro only): approx $36.74
· CPT 77402 (Level 1): approx $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approx $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approx $391.46 (PFS non-facility) to $564.51 (HOPPS)
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Delaware networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Delaware payment rates for CPT codes 77387, 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Delaware beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]
ATTN Missouri Medicaid - Payments for Radiation Therapy @OfficialRCCSInc
Josh Moore
Director, MO HealthNet
Missouri Department of Social Services
State of Missouri, Department of Social Services
615 Howerton Court, PO Box 6500
Jefferson City, MO 65102
[email protected]
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77387, 77402, 77407, and 77412
Dear Director:
I am writing to you in my capacity as Chairman of R3 and CEO of RC Billing with clients in Missouri to express grave concern regarding the current Missouri reimbursement rates for essential radiation oncology treatment delivery and guidance services. These outdated rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Missouri beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77387 (IGRT): $29.71
· CPT 77402 (Radiation treatment delivery, Level 1): $100.87
· CPT 77407 (Radiation treatment delivery, Level 2): $183.15
· CPT 77412 (Radiation treatment delivery, Level 3): $173.87
https://t.co/HrYFr5CcjV
These rates are catastrophically low and do not come close to covering the actual costs of delivering safe, precise, and effective radiation therapy. Radiation oncology requires substantial capital investment in linear accelerators, imaging systems, quality assurance, physics support, and highly trained clinical staff. At these reimbursement levels, practices cannot absorb the ongoing operational expenses, leading to reduced capacity, delayed treatments, or complete discontinuation of services for Missouri patients in many communities. This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care.
By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77387 (professional component only): approximately $36.74 (Medicare PFS non-facility; commercial payers often reimburse $100–$130)
· CPT 77402 (Level 1): approximately $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approximately $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approximately $391.46 (PFS non-facility) to $564.51 (HOPPS)
Missouri’s rates are lower than Medicare, creating an untenable disparity. These national rates at least allow practices to maintain operations and invest in modern technology required for accurate, image-guided treatment.
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Missouri networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Missouri payment rates for CPT codes 77387, 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
We are available to provide additional data, cost analyses, or meet with your team to discuss this matter promptly. Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Missouri beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]
Attn Connecticut Medicaid, VERY Low Radiation Therapy payments: @OfficialRCCSInc
Bill Halsey
Director, Division of Health Services
Connecticut Dept. of Social Services
55 Farmington Ave.
Hartford, CT 06105
[email protected]
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77387, 77402, 77407, and 77412
Dear Director:
I am writing to you in my capacity as Chairman of R3 and CEO of RC Billing with clients in Connecticut to express grave concern regarding the current Connecticut reimbursement rates for essential radiation oncology treatment delivery and guidance services. These outdated rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Connecticut beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77387 (IGRT): $ NOT Listed, Manually Priced
· CPT 77402 (Radiation treatment, Level 1): $62.65
· CPT 77407 (Radiation treatment, Level 2): $77.15
· CPT 77412 (Radiation treatment , Level 3): $90.87
These rates are catastrophically low and do not come close to covering the actual costs of delivering safe, precise, and effective radiation therapy. Radiation oncology requires substantial capital investment in linear accelerators, imaging systems, quality assurance, physics support, and highly trained clinical staff. At these reimbursement levels, practices cannot absorb the ongoing operational expenses, leading to reduced capacity, delayed treatments, or complete discontinuation of services for Connecticut patients in many communities. This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care.
By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77387 (professional component only): approximately $36.74 (Medicare PFS non-facility; commercial payers often reimburse $100–$130)
· CPT 77402 (Level 1): approximately $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approximately $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approximately $391.46 (PFS non-facility) to $564.51 (HOPPS)
Connecticut’s rates are lower than Medicare, creating an untenable disparity. These national rates, while not extravagant, at least allow practices to maintain operations and invest in modern technology required for accurate, image-guided treatment.
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Connecticut networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Connecticut payment rates for CPT codes 77387, 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
We are available to provide additional data, cost analyses, or meet with your team to discuss this matter promptly. Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Connecticut beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]
ATTN Wisconsin Medicaid, while it is nice that Wisconsin has agreed to update their IGRT and is now paying $28.14 for IGRT rather than $0, the overall rates below are still dismal in my opinion. Please get engaged: @OfficialRCCSInc
Amanda Dreyer
Medicaid Director
Wisconsin Department of Health Services
State of Wisconsin, Department of Health Services
1 West Wilson Street, Room 350 PO Box 309
Madison, WI 53701-0309
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77387, 77402, 77407, and 77412
Dear Medicaid Director:
I am writing to you in my capacity as Chairman of R3 and CEO of RC Billing with clients in Wisconsin to express grave concern regarding the current Wisconsin reimbursement rates for essential radiation oncology treatment delivery and guidance services. These outdated rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Wisconsin beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77387 (IGRT): $28.14
· CPT 77402 (Radiation treatment, Level 1): $56.36 PT1
· CPT 77407 (Radiation treatment, Level 2): $212.86 PT1
· CPT 77412 (Radiation treatment, Level 3): $304.86 PT1
https://t.co/K2hDWFzyqN
These rates are catastrophically low and do not come close to covering the actual costs of delivering safe, precise, and effective radiation therapy. Radiation oncology requires substantial capital investment in linear accelerators, imaging systems, quality assurance, physics support, and highly trained clinical staff. At these reimbursement levels, practices cannot absorb the ongoing operational expenses, leading to reduced capacity, delayed treatments, or complete discontinuation of services for Wisconsin patients in many communities. This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care.
By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77387 (professional component only): approximately $36.74
· CPT 77402 (Level 1): approximately $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approximately $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approximately $391.46 (PFS non-facility) to $564.51 (HOPPS)
Wisconsin’s rates are lower than Medicare creating an untenable disparity. These national rates, while not extravagant, at least allow practices to maintain operations and invest in modern technology required for accurate, image-guided treatment.
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Wisconsin networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Wisconsin payment rates for CPT codes 77387, 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
We are available to provide additional data, cost analyses, or meet with your team to discuss this matter promptly. Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Wisconsin beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]
@GavinNewsom Why are the republican districts having drop boxes burned? Why did you endorse such a poor candidate with a poor track record like Karen Bass? Is this more of you enabling FRAUD?
Attn Colorado Medicaid - Low $
Adela Flores-Brennan
Medicaid Director
Health First Colorado State of Colorado, Department of Health Care Policy and Financing; Medicaid & Child Health Plan
1570 Grant Street
Denver, Colorado 80203-1818
[email protected]
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77402, 77407, and 77412
Dear Medicaid Director:
I am writing to you in my capacity as Chairman of R3 and CEO of RC Billing with clients in Colorado to express grave concern regarding the current Colorado reimbursement rates for essential radiation oncology treatment delivery and guidance services. These outdated rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Colorado beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77402 (Radiation treatment, Level 1): $57.99
· CPT 77407 (Radiation treatment, Level 2): $68.35
· CPT 77412 (Radiation treatment, Level 3): $116.10
These rates for the treatment are catastrophically low and do not come close to covering the actual costs of delivering safe, precise, and effective radiation therapy. Radiation oncology requires substantial capital investment in linear accelerators, imaging systems, quality assurance, physics support, and highly trained clinical staff. At these reimbursement levels, practices cannot absorb the ongoing operational expenses, leading to reduced capacity, delayed treatments, or complete discontinuation of services for Colorado patients in many communities. This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care.
By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77402 (Level 1): approximately $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approximately $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approximately $391.46 (PFS non-facility) to $564.51 (HOPPS)
Colorado’s treatment materially rates are lower than Medicare’s creating an untenable disparity. These national rates, while not extravagant, at least allow practices to maintain operations and invest in modern technology required for accurate, image-guided treatment.
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Colorado networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Colorado payment rates for CPT codes 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
We are available to provide additional data, cost analyses, or meet with your team to discuss this matter promptly. Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Colorado beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]
https://t.co/IK1nM94j0i
@OfficialRCCSInc
Attn Wyoming Medicaid: @OfficialRCCSInc
Jesse Springer
Medicaid Director
Wyoming Department of Health
6101 Yellowstone Road, Suite 210
Cheyenne, WY 82009
Re: Urgent Request to Update and Correct Medicaid Payment Rates for Radiation Oncology Services – CPT® Codes 77387, 77402, 77407, and 77412
Dear Medicaid Director:
I am writing to you in my capacity as Chairman of R3 and CEO of RC Billing with clients in Wyoming to express grave concern regarding the current Wyoming reimbursement rates for essential radiation oncology treatment delivery and guidance services. These outdated rates are unsustainable, severely undermine the financial viability of providing high-quality radiation therapy, and place timely access to care at serious risk for Wyoming beneficiaries who require this life-saving treatment for cancer if these facilities are forced to halt services.
The rates for the revised radiation treatment codes are as follows:
· CPT 77387 (IGRT): $32.83 1/1/26
· CPT 77402 (Radiation treatment delivery, Level 1): $80.88 1/1/17
· CPT 77407 (Radiation treatment delivery, Level 2): $285.41 4/28/26
· CPT 77412 (Radiation treatment delivery, Level 3): $351.77 4/28/26
These rates are low and do not come close to covering the actual costs of delivering safe, precise, and effective radiation therapy. Radiation oncology requires substantial capital investment in linear accelerators, imaging systems, quality assurance, physics support, and highly trained clinical staff. At these reimbursement levels, practices cannot absorb the ongoing operational expenses, leading to reduced capacity, delayed treatments, or complete discontinuation of services for Wyoming patients in many communities. This directly jeopardizes patient outcomes in a vulnerable population that already faces barriers to care.
By comparison, national Medicare benchmarks for these same services (updated effective January 1, 2026, under the revised CPT coding structure that bundles technical image guidance into the delivery codes) are substantially higher and reflect the true resources involved:
· CPT 77387 (pro only): approximately $36.74
· CPT 77402 (Level 1): approx $79.49 (PFS non-facility) to $104.24 (HOPPS)
· CPT 77407 (Level 2): approx $317.64 (PFS non-facility) to $394.05 (HOPPS)
· CPT 77412 (Level 3): approx $391.46 (PFS non-facility) to $564.51 (HOPPS)
Wyoming’s rates are lower than Medicare’s creating an untenable disparity. Many commercial payers reimburse at even higher levels. These national rates, while not extravagant, at least allow practices to maintain operations and invest in modern technology required for accurate, image-guided treatment.
The situation is urgent. Radiation therapy is a cornerstone of curative and palliative cancer care in which approximately 60% of cancer patients receive radiation therapy at some point in their treatment journey. Inadequate reimbursement threatens provider participation in Wyoming networks, reduces geographic access (particularly in underserved areas), and risks poorer survival outcomes and increased downstream costs to the state from unmanaged disease progression.
We respectfully request that your appropriate team immediately review and align Wyoming payment rates for CPT codes 77387, 77402, 77407, and 77412 with national Medicare benchmarks (or a reasonable cost-based equivalent) to ensure continued access to these critical services.
We are available to provide additional data, cost analyses, or meet with your team to discuss this matter promptly. Thank you for your immediate attention to this critical patient-access issue. We look forward to your response and collaborative action to protect Wyoming beneficiaries’ access to radiation oncology care.
Sincerely,
Ron DiGiaimo MBA FACHE
Chairman of R3 and CEO of RC Billing
[email protected]