👁️✨ Un día como hoy, 5 de junio de 1862, nacía el médico sueco Allvar Gullstrand, el hombre que logró descifrar con precisión cómo viaja la luz dentro del ojo humano.
🤯 Gracias a sus investigaciones, hoy podemos diagnosticar y tratar enfermedades oculares con una precisión impensable en su época.
🔬 Diseñó instrumentos revolucionarios que transformaron la oftalmología y creó modelos tan exactos del ojo humano que muchos de sus principios siguen vigentes más de 100 años después.
🏆 Su impacto fue tan extraordinario que recibió el Premio Nobel de Medicina en 1911, siendo hasta hoy el único oftalmólogo que ha conseguido este reconocimiento.
👁️ Un hombre que nos ayudó, literalmente, a entender cómo vemos el mundo.
Transferrin: the vigilant iron courier of the bloodstream
Transferrin is a glycoprotein of about 80 kDa, synthesized mainly in the liver, that circulates in plasma as the main iron transport protein. Each transferrin molecule can bind two ferric ions (Fe³⁺) with high affinity, but only when these are coupled to bicarbonate, which serves as an anion bridge. The iron-binding sites are located in the two homologous lobes of the protein, each undergoing a conformational change upon metal binding—closing like a clam shell to protect the iron from unwanted redox reactions.
Biochemically, transferrin is part of the β-globulin fraction in electrophoresis and normally circulates at 2.0–3.6 g/L, with about one-third of its binding sites occupied (known as transferrin saturation, typically 20–40%). Its receptor, TfR1, is highly expressed in proliferating cells, especially in bone marrow erythroblasts, ensuring efficient delivery of iron for hemoglobin synthesis. Once the transferrin–iron complex binds the receptor, it is internalized into endosomes where the acidic pH releases the metal, and apotransferrin returns to plasma for another cycle.
Clinically, transferrin levels and saturation are key indicators of iron metabolism. High transferrin with low saturation suggests iron deficiency anemia, reflecting the liver’s attempt to capture scarce iron. Conversely, low transferrin levels occur in chronic inflammation, liver disease, malnutrition, or nephrotic syndrome. In hemochromatosis, saturation exceeds 60%, indicating iron overload. Measurement of transferrin or its iron-binding capacity remains an essential laboratory tool for diagnosing and monitoring disorders of iron balance.
This second instalment on FGF-2323 is devoted to one of its most fascinating partners occupying a remarkably central mechanistic position: Klotho.
Interestingly, even the name carries biological symbolism.
Klotho was named after Clotho, the youngest of the Three Fates in Greek mythology — the figure responsible for spinning the thread of life. The choice was not accidental. Mice lacking Klotho develop a striking premature ageing phenotype, with vascular calcification, osteoporosis, skin atrophy, sarcopenia and shortened lifespan, suggesting that this protein sits at the intersection of mineral metabolism and ageing itself.
BTW, the first chapter is here, https://t.co/qAH4U1zeWu
Klotho is not merely an accessory factor.
It is the obligatory co-receptor for FGF-23. Without Klotho, FGF-23 cannot effectively signal through its canonical FGFR1c pathway in the kidney or parathyroid gland.
Klotho determines whether FGF-23 functions as a coherent endocrine regulator or becomes a frustrated signal amplified into excess.
In early chronic kidney disease, Klotho expression — particularly in the distal nephron — declines very early, often before overt biochemical abnormalities appear. This creates a fascinating paradox:
- FGF-23 levels rise sharply, yet its phosphaturic efficiency progressively falls.
- The system responds by producing even more FGF-23, attempting to overcome resistance.
What appears clinically as “FGF-23 excess” is therefore, at least in part, a state of Klotho deficiency–induced endocrine resistance.
The implications for secondary hyperparathyroidism are layered.
1⃣ Reduced Klotho impairs FGF-23–mediated phosphate excretion, worsening phosphate retention — one of the major chronic stimuli for PTH synthesis and parathyroid hyperplasia.
2⃣ Klotho is also expressed in the parathyroid gland itself. Under physiological conditions, FGF-23 can suppress PTH secretion. But as Klotho expression declines in hyperplastic glands, this inhibitory pathway is progressively lost. The gland becomes resistant not only to vitamin D, but also to FGF-23.
3⃣ Soluble Klotho appears to exert direct modulatory effects on ion channels and calcium handling, potentially influencing parathyroid sensitivity to extracellular calcium, although this remains less clearly defined than its co-receptor role.
So where does Klotho sit in the hierarchy of renal hyperparathyroidism?
Not as the primary trigger in the classical sense — unlike phosphate retention or calcitriol deficiency — but as a permissive regulator that determines whether the endocrine network can still interpret its own signals correctly.
Klotho deficiency transforms an adaptive endocrine loop into a resistant one.
- FGF-23 rises.
- Phosphate accumulates.
- Calcitriol falls.
But progressively, the parathyroid gland stops listening.
What emerges is not merely overstimulation, but loss of regulatory coherence — one of the defining physiological features of advanced chronic kidney disease.
✅ El Gobierno aprueba 652 plazas nuevas para personal científico, t��cnico y de gestión en los Organismos Públicos de Investigación.
📈 La OPE 2026 de @CienciaGob supone un incremento de más del 8% respecto al año anterior en turno libre.
https://t.co/YMPnB2lWWL
It is often stated, almost reflexively, that modern transfusion medicine begins with Karl Landsteiner and his description of the ABO blood groups in 1901. Indeed, this discovery was crucial in rendering transfusion biologically intelligible and, crucially, immunologically safe. Yet, in strictly practical terms, Landsteiner’s work had no immediate clinical utility. Blood could now be matched, but it still could not be stored. Transfusion remained an improvised, high-risk procedure performed directly from donor to recipient—“arm to arm”—because coagulation rendered any collected blood unusable within minutes.
The true inflection point came not from immunohaematology, but from biochemical insight. In 1914, the Argentine physiologist Luis Agote demonstrated in Buenos Aires that the addition of a dilute sodium citrate solution prevented blood clotting ex vivo without inducing toxicity upon transfusion. This deceptively simple intervention fundamentally altered the temporal constraints of transfusion. Blood was no longer perishable within minutes; it became a storable biological material.
Almost concurrently, Albert Hustin and Richard Lewisohn reported similar findings. However, Agote’s work holds particular historical significance as the first publicly documented successful transfusion of stored human blood.
Only when citrate anticoagulation was combined with ABO compatibility did transfusion become both safe and operationally feasible. This convergence transformed transfusion from an experimental manoeuvre into a scalable medical practice. Its impact became immediately evident during the World War I, where the ability to store and transport blood saved innumerable lives and led to the establishment of the first rudimentary blood banks.
Subsequent advances—such as the identification of the Rh system and the introduction of plastic blood bags—refined the field, but did not redefine its foundation.
Landsteiner clarified compatibility.
Agote enabled applicability.
Without anticoagulation, the Nobel-winning discovery remained, for more than a decade, clinically inert. And the Prize had to wait until 1930.
His discovery was rejected.
His experiments were dangerous.
His conclusions contradicted everything chemists believed.
But, he was right.
At the beginning of the 19th century, Friedrich Sertürner isolated a crystalline compound from opium that would not only become the first modern analgesic, but also overturn one of the central assumptions of medicinal chemistry…
He named it Morphium, after Morpheus, the Greek god of dreams. What is critical here is not only the pharmacological activity, but the chemical nature of the compound.
At that time, the prevailing paradigm in pharmacognosy and early organic chemistry held that the “active principles” of medicinal plants were acidic in nature. This belief derived from earlier successes in isolating organic acids such as tartaric and citric acid, which reinforced a reductionist but ultimately flawed framework: biological activity was assumed to correlate with acidity.
Sertürner’s compound directly contradicted this dogma.
Morphine was not an acid—it was a basic, nitrogen-containing molecule, inaugurating what would later be defined as the class of alkaloids. This was a profound epistemological shift: it established that plant bioactivity could reside in organic bases, thereby expanding the chemical landscape of pharmacologically active compounds.
Equally transformative was the fact that Sertürner isolated morphine in a pure, crystalline form.
For the first time, a drug derived from a plant could be quantified, titrated, and administered with controlled dosing. This marked a decisive transition from empirical phytotherapy—where variability in plant extracts led to unpredictable effects—to a proto-pharmacological model grounded in dose–response relationships.
Sertürner himself explored these relationships experimentally, in a manner that today would raise serious ethical concerns but was methodologically revealing. He conducted self-experiments and trials on acquaintances, administering measured doses of morphine.
Through these observations, he described a clear dose-dependent progression of effects: at lower doses, morphine induced euphoria and analgesia; as the dose increased, these effects transitioned into dizziness and somnolence; and with approximately doubled concentrations, profound sedation and sleep ensued.
These observations constitute one of the earliest documented characterizations of a graded pharmacodynamic response, anticipating the modern concept of therapeutic windows and toxicity thresholds.
Despite the robustness of his findings, Sertürner’s initial publications were met with skepticism and even rejection.
His conclusions challenged entrenched chemical doctrine, and the notion that a basic compound could be the principal active agent of opium was considered implausible.
The resistance he encountered reflects the inertia of scientific paradigms: evidence alone is often insufficient when it conflicts with established theoretical frameworks.
Only after repeated publications, broader dissemination, and independent confirmation did the scientific community begin to accept his work.
The implications were far-reaching.
Morphine became the prototype for a new class of compounds, and its discovery catalyzed the isolation of other alkaloids such as quinine, strychnine, and caffeine.
More importantly, it established a new principle: that specific physiological effects can be attributed to discrete, chemically defined molecules, whose activity depends on dose and molecular structure.
Thus, the isolation of morphine was not simply the discovery of a powerful analgesic—it was the collapse of a chemical dogma and the birth of molecular pharmacology.
It redefined how drugs were conceptualized, studied, and administered, and it introduced a quantitative, experimental approach that remains foundational in biomedical science.
Tal día como hoy, el 1/3/1852, nació Henri Becquerel, el físico francés que descubrió la radiactividad por una de las casualidades más famosas de la ciencia.En 1896, intrigado por los recién descubiertos rayos X, quiso comprobar si las sales de uranio emitían algo parecido al exponerse a la luz solar. Colocó cristales de uranio sobre placas fotográficas envueltas en papel negro (para que no entrara luz) y las dejó preparadas para un día soleado. Pero el clima en París se nubló varios días seguidos. Sin poder hacer el experimento como planeaba, guardó todo en un cajón oscuro.Días después, decidió revelar las placas “por probar”… y ahí estaba lo inesperado: estaban fuertemente impresionadas, como si hubieran recibido luz intensa. El uranio había emitido radiación por sí solo, sin sol, sin estímulo externo. La energía venía del interior del átomo.Ese hallazgo sería profundizado por y , que aislaron nuevos elementos radiactivos y dieron nombre al fenómeno: radiactividad.Hoy, aquel “experimento fallido” es la base de la radioterapia que destruye tumores con precisión, de la medicina nuclear que detecta cáncer y enfermedades cardíacas en fases tempranas y de múltiples técnicas diagnósticas esenciales en hospitales de todo el mundo.Un cajón cerrado. Unos días nublados. Y una revolución que aún salva vidas.
Is citrulline a better surrogate for kidney function than creatinine?
*⃣ Creatinine has long been the pragmatic cornerstone for estimating glomerular filtration rate (GFR). It is generated at a relatively constant rate from creatine phosphate in skeletal muscle, freely filtered at the glomerulus, and only modestly secreted by proximal tubules.
*⃣ Citrulline offers a conceptually different lens on renal function.
It is a non-proteinogenic amino acid synthesised almost exclusively by small intestinal enterocytes from glutamine and proline.
In proximal tubular cells, citrulline is taken up and converted to arginine via argininosuccinate synthetase and lyase, directly linking renal citrulline handling to nitric oxide biology and nitrogen balance.
*⃣ From a physiological perspective, this gut–kidney axis is what makes citrulline attractive.
Importantly, citrulline production is independent of muscle mass and largely unaffected by dietary protein intake, theoretically reducing the confounding that plagues creatinine-based estimates.
In advanced renal failure, impaired renal uptake and metabolism become the dominant determinant of circulating citrulline levels.
*⃣ Citrulline is not merely cleared by the kidney; it is metabolically transformed by it. Thus, plasma levels reflect tubular metabolic capacity as much as filtration.
Moreover, enterocyte mass is a critical upstream determinant. Conditions such as short bowel syndrome, severe mucositis, coeliac disease, or intestinal failure markedly lower citrulline concentrations, irrespective of renal function, undermining specificity in multisystem disease.
*⃣ Assays are less standardised, reference intervals are poorly harmonised, and large-scale validation against gold-standard GFR measurements across CKD stages is limited.
*⃣ At present, its strongest promise may lie not in replacement but in complementation: as part of multimarker strategies capturing filtration, tubular metabolism, and systemic physiology.
In summary, citrulline is biologically elegant and mechanistically informative, but not yet superior.
Creatinine remains clinically dominant because of its deep validation and operational simplicity.
Is citrulline a better surrogate for kidney function than creatinine?
1⃣ Creatinine has long been the pragmatic cornerstone for estimating glomerular filtration rate (GFR).
▶️ It is generated at a relatively constant rate from creatine phosphate in skeletal muscle, freely filtered at the glomerulus, and only modestly secreted by proximal tubules.
▶️ Yet its apparent simplicity masks important physiological noise. Muscle mass, age, sex, diet, ethnicity, and drugs affecting tubular secretion all shape serum creatinine concentrations, blunting sensitivity to early nephron loss and complicating interpretation in sarcopenic, elderly, critically ill, or oncological patients.
2⃣ Citrulline offers a conceptually different lens on renal function.
▶️ It is a non-proteinogenic amino acid synthesised almost exclusively by small intestinal enterocytes from glutamine and proline.
▶️ Unlike most amino acids, citrulline largely escapes hepatic uptake and enters the systemic circulation, where the kidney becomes its primary site of metabolism.
▶️ In proximal tubular cells, citrulline is taken up and converted to arginine via argininosuccinate synthetase and lyase, directly linking renal citrulline handling to nitric oxide biology and nitrogen balance.
3⃣ From a physiological perspective, this gut–kidney axis is what makes citrulline attractive.
▶️ Plasma citrulline concentrations rise as renal function declines, showing an inverse relationship with measured GFR.
▶️ Importantly, citrulline production is independent of muscle mass and largely unaffected by dietary protein intake, theoretically reducing the confounding that plagues creatinine-based estimates.
▶️ In advanced renal failure, impaired renal uptake and metabolism become the dominant determinant of circulating citrulline levels.
4⃣However, this same biology introduces complexity.
▶️ Citrulline is not merely cleared by the kidney; it is metabolically transformed by it. Thus, plasma levels reflect tubular metabolic capacity as much as filtration.
▶️ Moreover, enterocyte mass is a critical upstream determinant. Conditions such as short bowel syndrome, severe mucositis, coeliac disease, or intestinal failure markedly lower citrulline concentrations, irrespective of renal function, undermining specificity in multisystem disease.
5⃣ Analytically, citrulline also lags behind creatinine.
▶️ Assays are less standardised, reference intervals are poorly harmonised, and large-scale validation against gold-standard GFR measurements across CKD stages is limited.
6⃣ At present, its strongest promise may lie not in replacement but in complementation: as part of multimarker strategies capturing filtration, tubular metabolism, and systemic physiology.
In summary, citrulline is biologically elegant and mechanistically informative, but not yet superior.
▶️ Creatinine remains clinically dominant because of its deep validation and operational simplicity.
▶️ Citrulline’s future likely resides in refined phenotyping of renal dysfunction, rather than routine substitution.
Ante tanta desinformación sobre la efectividad de la vacuna de la gripe de esta temporada y dirigido a medios de comunicación serios, va un 🧵resumiendo los puntos clave del reciente informe de @ECDC_EU
Esta vez agradezco 🔁 para que llegue al mayor número de personas posible.
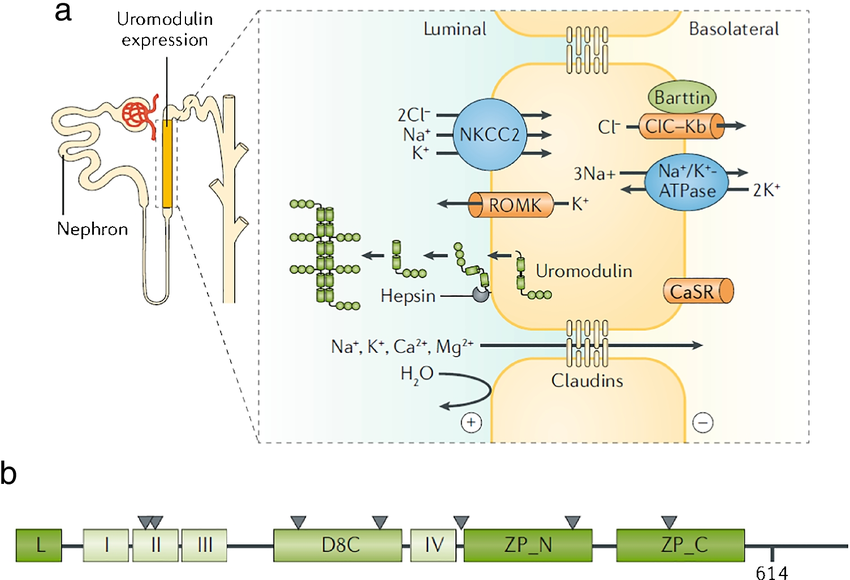
The most abundant protein in urine isn’t waste — it’s a guardian. I am talking about uromodulin, the kidney’s secret protein with a dual identity.
🌟 Uromodulin, aka Tamm–Horsfall protein, is the most abundant protein in normal human urine — yet for decades its function remained mysterious.
1⃣ It is produced exclusively by the epithelial cells of the thick ascending limb of the loop of Henle and released into the tubular lumen after cleavage of its glycosylphosphatidylinositol (GPI) anchor.
2⃣ Structurally, uromodulin is a large, heavily glycosylated protein that polymerises into long filaments, forming a molecular mesh that coats the urinary tract. Its unique architecture underpins both its protective and pathological roles.
3⃣ Physiologically, uromodulin is a molecular sentinel. ▶️ Its carbohydrate side chains bind to type 1 fimbriae of Escherichia coli, preventing the bacteria from attaching to urothelial cells — effectively a “decoy receptor” defence against urinary tract infection.
▶️ It also inhibits calcium crystal aggregation, lowering the risk of nephrolithiasis by maintaining solubility in supersaturated urine.
▶️ Additionally, when secreted basolaterally into the interstitium, uromodulin interacts with immune cells, modulating inflammation and maintaining local tolerance.
4⃣ However, this same protein becomes pathogenic when its folding is disrupted by genetic mutations.
▶️ In familial juvenile hyperuricaemic nephropathy (FJHN) and related uromodulin-associated kidney diseases, missense mutations in the UMOD gene cause misfolding and intracellular retention of uromodulin within the endoplasmic reticulum.
This triggers a chronic unfolded protein response, leading to tubular cell stress, interstitial fibrosis, and progressive renal failure.
The associated hyperuricaemia arises from impaired sodium and urate handling in the thick ascending limb.
5⃣ Uromodulin thus embodies a molecular duality:
▶️ When properly folded and released, it shields the kidney from infection and crystal injury.
▶️ When misfolded and trapped, it slowly destroys it from within.
6⃣ Current research explores whether serum uromodulin levels can serve as a biomarker of nephron health — a secret from the kidney that may help diagnose its own decline.
Its story also exemplifies how the same molecule can link innate immunity, tubular transport physiology, and genetic disease into a single molecular narrative.
#Physiology_RS #Nephro_RS
#Physiology #Nephrology
When FOXP3 stops working, the peace-keepers of the immune system vanish — and the war on self begins.
🌟 And the 2025 Nobel Prize in Physiology or Medicine was awarded to Mary E. Brunkow, Fred Ramsdell and Shimon Sakaguchi because their work illuminated how the immune system spares our own tissues — with FOXP3 and regulatory T cells (Tregs) at the heart of that mechanism.
1⃣ FOXP3 (Forkhead box P3) is one of the most emblematic transcription factors in immunology — a master regulator that decides whether a T cell will become a fierce warrior or a peacekeeper.
2⃣ Biochemically, contains a zinc finger and a leucine zipper domain, allowing it to dimerize and interact with other transcriptional regulators, enabling FOXP3 to reprogram gene expression, suppressing effector functions and enforcing the identity of Tregs.
3⃣ Once expressed, FOXP3 stabilizes the Treg lineage by activating genes such as CTLA-4, CD25, and GITR, while repressing those typical of effector T cells like IL-2, IFN-γ, and IL-17.
4⃣ Binds DNA and recruits chromatin-modifying complexes, including histone acetyltransferases and deacetylases, to remodel chromatin architecture and impose a suppressive transcriptional program.
This “epigenetic lockdown” ensures that Tregs remain tolerant and stable even when exposed to inflammatory signals.
5⃣ In their absence, the immune system spirals into chaos. The clearest example of this is the rare but devastating IPEX syndrome (Immunodysregulation, Polyendocrinopathy, Enteropathy, X-linked), caused by mutations in FOXP3. Children with IPEX develop severe autoimmunity affecting the gut, pancreas, skin, and thyroid, usually within the first months of life — a striking demonstration that immune tolerance depends on one single gene.
FOXP3 is not just another transcription factor; it is the molecular signature of peace in the immune system — the voice that tells T cells when to fight and when to stand down. Without it, the body turns its weapons inward, proving that immune equilibrium depends on biochemical restraint as much as on defense.
#Immunology_RS #Tolerance_RS #Immunology #Tolerance
Plasma proteins are an enormous and diverse family — hundreds of different molecules (yes, that’s correct) — each designed for a very specific task. Together, they turn plasma into a dynamic biochemical network that maintains homeostasis, transports substances, defends against infections, and regulates osmotic pressure.
Let’s begin this series with albumin (#Plasma_RS, delivered one per week), the most abundant plasma protein, accounting for about 60% of total plasma protein mass.
Produced exclusively by the liver, human serum albumin is a single polypeptide chain of roughly 66 kDa. Its compact globular structure contains multiple hydrophobic and hydrophilic pockets, making it one of the most versatile carrier proteins in biology.
At the molecular level, albumin binds and transports a wide variety of molecules — neutral, positively, and negatively charged compounds alike. Thanks to its amphipathic nature, it carries non-polar molecules such as fatty acids, cholesterol, and many lipophilic drugs, as well as polar or charged substances like bilirubin, ions (notably calcium), and hormones including thyroxine and cortisol. The binding is reversible, acting as a reservoir and regulator of these molecules’ plasma concentration and bioavailability.
Physiologically, albumin’s most critical role is maintaining oncotic (colloid osmotic) pressure, preventing plasma water from escaping into interstitial spaces. Low albumin levels — from liver disease, nephrotic syndrome, or malnutrition — lead to edema and ascites.
Despite its small size, albumin is negatively charged at physiological pH, which prevents it from being freely filtered through the glomerular membrane. In healthy kidneys, less than 0.01% of plasma albumin crosses the glomerulus, and most of that is reabsorbed by proximal tubule cells. Detectable albumin in urine (albuminuria) is therefore an early marker of glomerular damage.
Normally, plasma contains about 35–50 g/L of albumin, with a globulin-to-albumin ratio (A/G ratio) of approximately 1.5:1. This delicate balance reflects the liver’s synthetic capacity and the integrity of the vascular and renal systems.
In short, albumin is not a passive bystander but a molecular multitasker — a negatively charged, amphipathic protein that stabilizes the internal milieu, ferries molecules across the plasma, buffers pH, and silently guards the body’s osmotic equilibrium.
#Physiology_RS #Blood_RS
En plena Segunda Guerra Mundial, armada con rayos X y una mente brillante, Dorothy Hodgkin iba a revolucionar la medicina, porque su trabajo salvaría millones de vidas. Dorothy desentrañó la estructura de la penicilina, permitiendo su producción masiva. Tira del hilo 🧵👇🏽👇🏽👇🏽
Año 1963.
Dos tubos de ensayo. Dos personas que jamás se conocieron: un joven aborigen australiano y un paciente hemofílico en Nueva York.
Alguien mezcla sus muestras.
Y algo imposible sucede. Algo que cambió la #HistoriaMedicina 🧵⤵️
En su primer disco la banda aglutinó influencias y absorbió el papel de precursores como Deep Purple o Led Zeppelin para crear algo nuevo.
Crearon un genero que es más que música para millones de personas en todo el mundo.
Es una forma de vida.
No escuchas heavy.
Eres heavy.
'El apagón fue más complejo de lo que crees'. Detallado análisis de @Astrofriki en su canal de YouTube: https://t.co/dIvOhbsal0
Fragmento sobre el papel de la energía nuclear en el apagón.