📱🫁Utilidad del PoCUS en el Manejo del Embolismo Pulmonar con Inestabilidad Hemodinámica
🔰📚Critical Care 2026
https://t.co/ZscgQ8HpX6
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/rPEDXf5xvO
😵💫🩸Mecanismos, Abordaje y Manejo de la Encefalopatía Urémica
🔰📚Kidney International
https://t.co/W52itklf1G
Enlace a Articulo Completo👇🏻✅🆓
https://t.co/rPEDXf5xvO
🫀🫁PoCUS Cardio - Pulmonar en el Manejo de la Disnea Indiferenciada
🔰📚JAMA 2025
doi:10.1001/jamanetworkopen.2025.30677
Enlace a Articulo Completo👇🏻✅🆓
https://t.co/xumUMHaxVK
Hay que conocer sobre fisiología y patología solamente para saber algo y ser menos idiota.
Pero la teoría no siempre se traduce literalmente a la clínica.
En teoría la vitamina C fomenta la producción de colágena por lo que suelen darla a los quemados..
https://t.co/x9Qi5Wt6rn
🫀⚙️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤𝙥𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada
🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
https://t.co/S4Hy5iDXf0
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd
Platicando con mi compañera de vida comentamos que muchas veces los médicos cargan con sus decesos: los Psiquiatras con los suicidios, los Ginecos con los bebés, los Clínicos acompañan a sus pacientes hasta la muerte, los quirúrgicos tomando decisiones de rápida para no complicarse. Algunos se enfrían en el camino la disociación o la falta de empatía los protege y ya vienen distanciados a la condición humana pero siendo buenos técnicos. Otros más sensibles es un golpe irreparable y más en las condiciones que se presenta, inevitable no mezclar el sentido de responsabilidad y la culpa asómandose en el sótano. Pero tienes que seguir. Los riesgos de esta profesión son muchos pero alguien tiene que hacer este trabajo y muchas veces no se sabe como lidiar con esos procesos tan complejos. Algunos se malignizan y otros se vulnerabilizan.
Today's Paper of the Day is:
Protective nutrition strategy in the acute phase of critical illness: why, what and how to protect
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
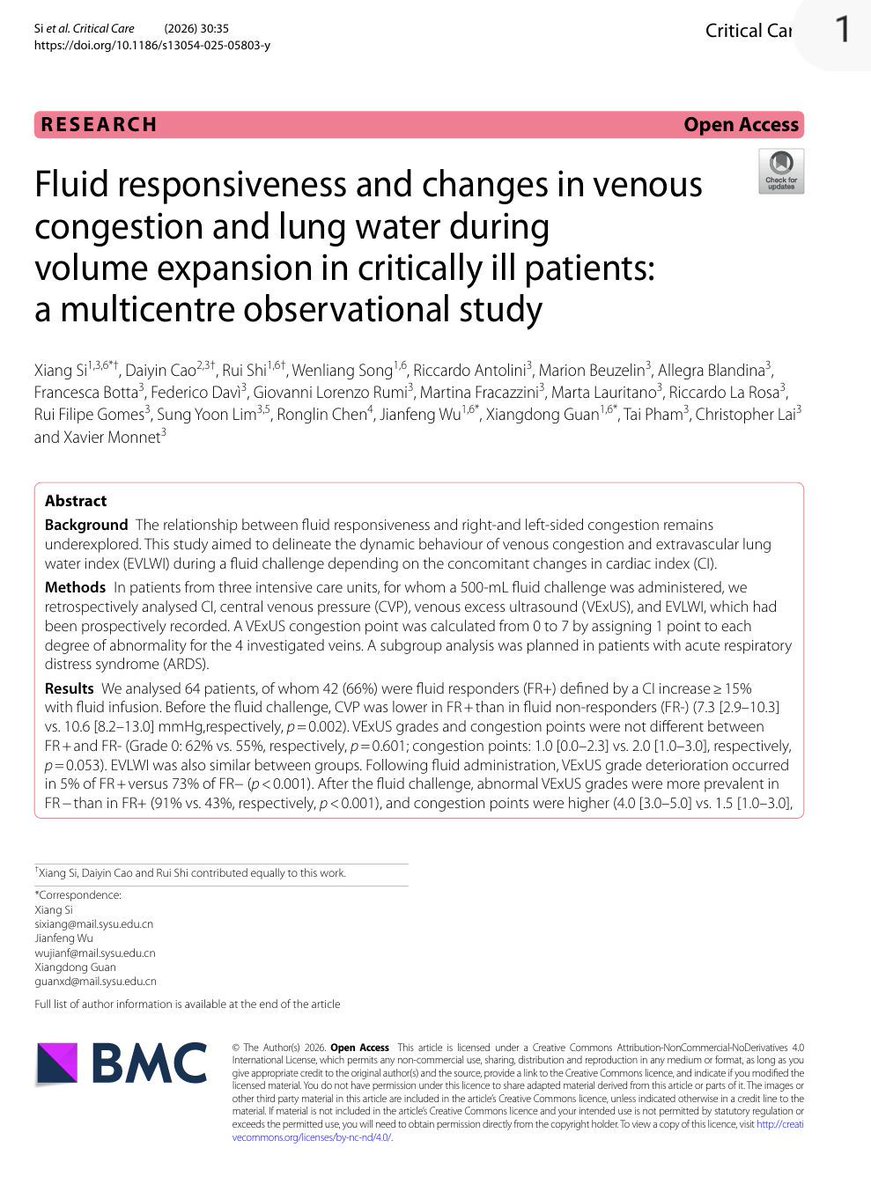
💧 Fluid Responsiveness ≠ Fluid Tolerance
For years, critical care clinicians have focused on a fundamental question:
Will this patient increase cardiac output if I give fluids?
A new multicentre study from France and China suggests we may need to ask a second question:
What price will the patient pay for that fluid?
In this observational study of 64 critically ill patients receiving a standardized 500 mL fluid challenge, investigators evaluated not only cardiac index (CI), but also venous congestion using VExUS and pulmonary congestion using extravascular lung water (EVLWI).
The findings are striking.
Before fluid administration, venous congestion could coexist with fluid responsiveness. In fact, many patients remained preload responsive despite already demonstrating evidence of systemic venous congestion.
However, what happened after fluid administration was even more important.
Among fluid responders:
✅ Cardiac index increased significantly
✅ Venous congestion remained largely stable
✅ Only 5% experienced worsening VExUS grade
✅ Lung water remained relatively unchanged
Among fluid non-responders:
❌ Cardiac output barely changed
❌ Venous congestion worsened dramatically
❌ VExUS deterioration occurred in 73%
❌ EVLWI increased significantly
❌ Congestion became evident across hepatic, portal, and renal venous territories
Perhaps the most important physiological message is this:
When the heart cannot convert preload into flow, the fluid has to go somewhere.
And where it goes is congestion.
The study also found a strong correlation between CVP and VExUS, suggesting that while advanced ultrasound provides valuable organ-level information, a carefully interpreted CVP may still remain a useful bedside marker of right-sided congestion.
The ARDS subgroup provides another important lesson.
Even fluid-responsive ARDS patients accumulated more extravascular lung water after fluid administration than non-ARDS patients, highlighting the role of pulmonary permeability in determining fluid tolerance.
This study reinforces a concept that is increasingly central to modern hemodynamic management:
The goal is not simply to identify fluid responsiveness.
The goal is to identify patients who are both:
✔ Fluid responsive
✔ Fluid tolerant
A fluid challenge that increases congestion without increasing flow is not resuscitation.
It is fluid accumulation.
The future of hemodynamic management may lie at the intersection of:
• Fluid responsiveness
• Venous congestion assessment
• Pulmonary permeability
• Organ-specific fluid tolerance
Because the best fluid is not the one that can be given.
It is the one that provides benefit without causing harm.
Reference , 📚
Si X, Critical Care. 2026;30:35.
🫁🦠Abordaje y Manejo de la Neumonia Asociada a Ventilación Mecánica
🔰📚Infect Dis Clin
https://t.co/YZCRND2npc
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
🆕💥🔴Review summarizes recent clinical trials for treatment of tuberculous meningitis
🔺Disappointing Results high dose Rifampin HARVEST
🔺The only adjunctive therapy supported by trials to date is dexamethasone ( benefits may not be universal: HIV+, ACT HIV, no survival benefit)
🔺Several ongoing large trials investigating high dose rifampicin, with linezolid or moxifloxacin or enhanced dose isoniazid.
https://t.co/aZpLVrLVHn
PREVENCIÓN DE INSUFICIENCIA CARDÍACA
Documento ESC
🔴La mejor forma de reducir la morbilidad y ⚰️ por IC reside en la prevención
🔴Priorizar el manejo y tratamiento precoz de los factores de riesgo tradicionales (Sd Cardio-Reno-Metabólico)
🔴Factores de riesgo menos reconocidos que también debemos considerar
🔴Individualizar y estimar el riesgo de cada uno de nuestros pacientes
Vía @ESC_Journals
💉🫀Manejo Efectivo del Shock - Desde la Fisiología Hasta la Medicina Personalizada
🔰📚Critical Care Medicine
DOI: 10.1097/CCM.0000000000007115
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/rPEDXf5xvO
🧠🦠Manual Práctico de la OMS Para el Diagnóstico y Manejo de la Meningitis
🔰📚World Health Organization 2026
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK










![MarlonVFZR's tweet photo. 🫀⚙️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤𝙥𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HKX63pHWEAA2_2p.jpg)






















![MarlonVFZR's tweet photo. 🫀⚙️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤𝙥𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HKX63qOXIAA7-Go.jpg)