🆕 article in Anesthesiology Open! “Understanding Anesthesiologists’ Adoption of Evidence-based Neuromuscular Monitoring and Reversal Best Practices.”
Read the article: https://t.co/LeqoRRrS5F
⚡ Post-reperfusion syndrome complicates up to 77% of liver transplants. Cold, acidotic, hyperkalaemic blood returning to the heart can trigger arrhythmias and arrest. Anticipate it, augment the MAP, correct electrolytes.
Read more: https://t.co/5cvLdOfwMO
Llevo 3 años estudiando inglés y nadie me dijo esto.
Los phrasal verbs no se memorizan. Se entienden.
180 de los más usados, explicados de forma que por fin tienen sentido 👇
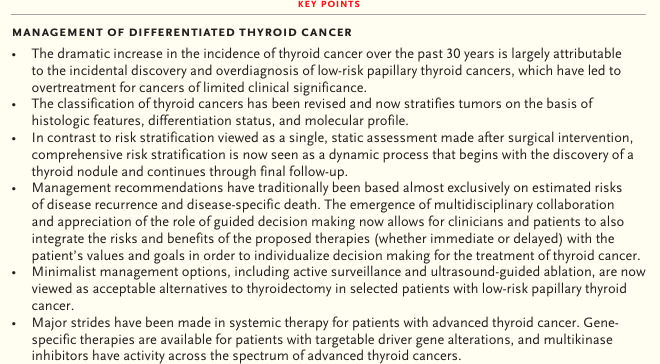
New England Journal of Medicine (NEJM) 2026: Manejo del cáncer de tiroides diferenciado
DOI:10.1056/NEJMra2416814
#MedEd#MedTwitter#MedX
https://t.co/cL7saZNryb
Suenas básico en inglés y no te das cuenta
1. Wait a minute → Hold on a sec
2. I agree → I'm on the same page
3. Stop it → Cut it out
4. I disagree → I'm not convinced
5. I'm tired → I'm exhausted
6. I'm busy → I'm tied up
7. I'm hungry → I'm starving
8. I'm happy → I'm delighted
9. I'm sad → I'm heartbroken
10. I'm scared → I'm terrified
11. I'm angry → I'm furious
12. I'm confused → I'm puzzled
13. I'm ready → I'm all set
14. I'm leaving → I'm heading out
15. I'm not sure → I'm uncertain
16. I don't know → I have no clue
17. It's easy → It's effortless
18. It's difficult → It's challenging
19. Hurry up → Pick up the pace
20. I'm listening → You have my full attention
Jiang, Ledowski, and Sleigh examine the evolving concept of intraoperative nociception, its underlying physiologic and neurobiological mechanisms, consequences, and the clinical strategies employed to assess and optimize antinociception regimens.
🔗 https://t.co/IfTehQEm9D
🍻Liver Disease and General Anesthesia: What Every Anesthesiologist Should Know in 2026
Patients with liver disease represent one of the highest-risk populations encountered in perioperative medicine. A recent review highlights how the evolving epidemiology of liver disease, particularly the rise of metabolic dysfunction-associated steatotic liver disease (MASLD), is reshaping anesthetic practice.
Key Clinical Messages
• Liver disease is associated with approximately a five-fold increase in 90-day postoperative mortality.
• MASLD has become the most common cause of chronic liver disease worldwide and is frequently undiagnosed during preoperative assessment.
• Perioperative risk is determined not only by hepatic dysfunction but also by associated cardiovascular, renal, metabolic, respiratory, and neurologic complications.
• Patients with cirrhosis often exhibit a paradoxical physiology: relative intravascular hypovolemia despite total body fluid overload, making hemodynamic management particularly challenging.
• Conventional coagulation tests (INR, PT, platelet count) do not accurately predict bleeding risk in cirrhosis. Viscoelastic testing (ROTEM/TEG) provides a more physiologically relevant assessment and can reduce unnecessary transfusions.
Preoperative Priorities
A comprehensive assessment should include:
✓ Child-Pugh and MELD/MELD-Na scoring
✓ Evaluation for portal hypertension and ascites
✓ Screening for cirrhotic cardiomyopathy
✓ Renal function and hepatorenal syndrome assessment
✓ Identification and treatment of hepatic encephalopathy
✓ Nutritional assessment for sarcopenia and malnutrition
✓ Cardiovascular risk stratification, especially in MASLD patients
The review emphasizes that elective procedures should be deferred in patients with acute liver failure or advanced acute-on-chronic liver failure whenever possible.
Intraoperative Considerations
Current evidence supports:
• Balanced crystalloids as first-line fluids
• Avoidance of excessive saline administration
• Careful albumin use in selected hypoalbuminemic patients
• Early invasive hemodynamic monitoring in advanced disease
• Norepinephrine as the preferred vasopressor when vasopressor support is required
• Restrictive transfusion strategies (target hemoglobin generally >7 g/dL)
• Lung-protective ventilation strategies
• Individualized dosing of hepatically metabolized drugs
Long-acting benzodiazepines should generally be avoided, opioids require cautious titration, and neuromuscular blockade monitoring becomes particularly important.
Reference 📚
Flick M, Current Opinion in Anaesthesiology. 2026;39(3):390–400. DOI: 10.1097/ACO.0000000000001648.
We are pleased to share that the BJA has received its Impact Factor of 10.3 for 2025, according to the latest Journal Citation Reports. This places the BJA first in the Anesthesiology category.
We thank our international team of authors, reviewers, editors and readers!
📌 Featured in UIA Vol. 42:
This article explores how PBM is being implemented across different health systems worldwide 🌍🩸
📖: https://t.co/YHfMvKvuTW
✍️By: Angel A. Pérez-Calatayud, Angel F. Galvan García, Carolina Haylock Loor, Seema Ranade, Rodrigo Rubio-Martínez, Naima Yusuf-Zakaria and Fredy Ariza
🫀Retorno venoso 🆚️ función cardíaca: ¿Quién impulsa realmente la circulación?
Cecconi,Ostermann, Pinsky
☝🏻🤓Durante décadas se enseñó que el corazón era el principal "motor" de la circulación. Sin embargo, la fisiología moderna integrando los conceptos de Guyton, Pinsky, Magder, Monnet y Teboul demuestra que el gasto cardíaco resulta del equilibrio dinámico entre la capacidad del corazón para bombear y la capacidad del sistema venoso para retornar sangre al corazón. La pregunta correcta no es quién domina, sino cómo interactúan ambos sistemas. 🫀
❤️ El corazón no puede bombear lo que no recibe.En estado estable:
▪️Retorno venoso (RV) = Gasto cardíaco (GC)
🔴La circulación se encuentra en el punto de intersección entre:
▪︎Curva de función cardíaca (Frank-Starling).
▪︎Curva de retorno venoso (Guyton).
🫀El flujo final depende del sistema más limitante.
☝🏻🤓Determinantes del retorno venoso: Ecuación de Guyton
▪️VR={Pms-PRA) /RVR
1. Presión media sistémica de llenado (Pms)
🕵♂️Es la presión generada por el volumen "estresado" del sistema venoso... y☝🏻🤓 Aumenta con:
●Expansión de volumen.
●Venoconstricción simpática.
●Norepinefrina.
☝🏻🤓Disminuye con:
●Hipovolemia.
●Vasoplejía séptica.
●Normal = 7-10 mmHg.
2. Presión auricular derecha (PRA o PVC). Es la contrapresión al retorno venoso.
● ↑ PVC → ↓ gradiente de retorno venoso.
⚠️Importante:
●La PVC elevada no significa necesariamente más precarga útil; frecuentemente representa congestión.🚿
3. Resistencia al retorno venoso (RVR).
●Depende principalmente de:
▪︎Arteriolas.
▪︎Microcirculación.
▪︎Vasomotricidad.
🫀La vasodilatación séptica puede reducir la RVR y aumentar inicialmente el gasto cardíaco.
🔴La función cardíaca
🫀El corazón responde al retorno venoso mediante:
▪️Mecanismo de Frank-Starling
🔴Si existe reserva de precarga:
▪️. ↑ retorno venoso → ↑ volumen sistólico.🫀
☝🏻🤓Pero cuando el corazón está en la porción plana de Starling:
▪️Más volumen → ↑ PVC y congestión, sin incremento del GC.
🫀¿Quién impulsa la circulación?
☝🏻🤓La respuesta moderna es:
Ambos.‼️
▪️El sistema venoso genera el gradiente de flujo.🩸🩸
▪️🫀El corazón determina cuánto de ese flujo puede ser eyectado.
🔴Si uno falla, el flujo disminuye.
📖Aplicación clínica en CHOQUE
🩸🔴Shock hipovolémico
⚠️Problema predominante:
▪️⬇ Pms
🔴🦠Shock séptico precoz
⚠️Problemas:
▪️↓ Pms (vasoplejía).
▪️↓ RVR.
🫀Miocardiopatía séptica variable.
●TX
✓ Norepinefrina temprana.
✓ Líquidos en pacientes respondedores.
✓ Dobutamina si existe disfunción miocárdica.
🔴🫀Shock cardiogénico
⚠️Problema principal:
▪️↓ pendiente de la curva cardíaca.
🚿La PVC aumenta y el retorno venoso encuentra una contrapresión elevada.
▪️Tratamiento:
✓ Inotrópicos. ✓ Reducción de poscarga. ✓ Soporte mecánico.
🚿Más volumen generalmente empeora la situación.
🔴El papel de la norepinefrina
▪️La norepinefrina no es solamente un vasopresor arterial.
Produce:▪️Venoconstricción
▪️⬆ Volumen estresado.
▪️⬆ Pms.
▪️⬆ Gradiente de retorno venoso.
▪️Puede ejercer cierto efecto inotrópico β1.
🦠Por ello, en shock séptico temprano puede aumentar el gasto cardíaco incluso antes de administrar grandes cantidades de líquidos. 💧💧
🔴Dobutamina y retorno venoso
🫀La dobutamina:Aumenta la contractilidad☝🏻🤓
🫀Incrementa la pendiente de la curva cardíaca.
🫀Disminuye la presión auricular derecha.
🫀Reduce la poscarga pulmonar.
✅️Favorece el retorno venoso.
☝🏻🤓Por ello, su efecto es más complejo que simplemente "aumentar la contractilidad".
☝🏻🤓Presión venosa central: una interpretación moderna
▪️La PVC debe verse como:
▪️La contrapresión del retorno venoso.
🚿Una PVC elevada significa:
🚿Congestión.
▪️Aumento de presión retrógrada.
▪️Disminución del gradiente Pms-PVC.
🔴Más que una medida de volumen.
La PVC no es una medida de precarga; es una medida de cuánto está dificultado el retorno venoso.
☝🏻🤓Actualizaciones 2024-2026
▪️Monnet y Teboul
📜La fisiología de Guyton sigue siendo válida y ayuda a explicar:
👇🏽
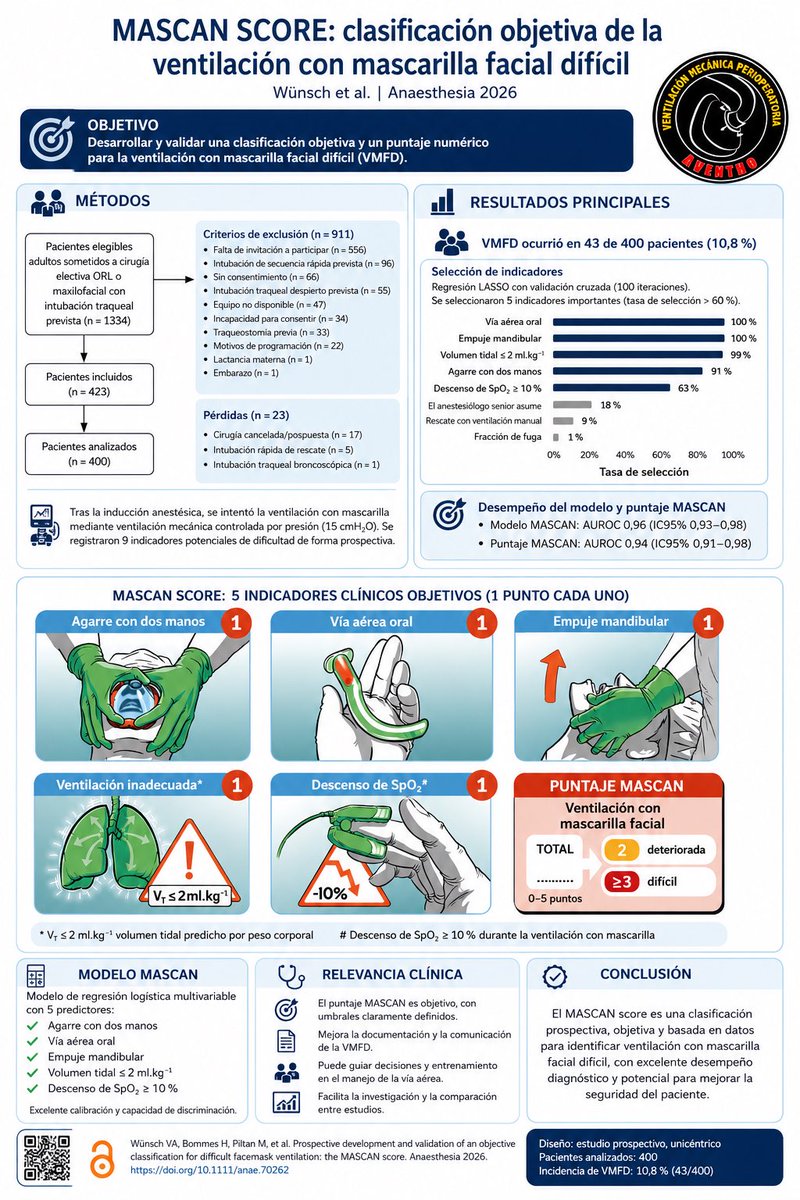
¿Ventilación con mascarilla facial difícil? El problema empieza por la definición
#AventhoAnestesia#Aventho#SMMCE#SAML
Durante años, la ventilación con mascarilla facial difícil ha sido una de las complicaciones más frecuentes y, al mismo tiempo, peor definidas del manejo de la vía aérea. Dependiendo de la definición utilizada, su incidencia puede variar desde <1% hasta más del 15%.
El estudio MASCAN propone un cambio importante: sustituir definiciones subjetivas como “ventilación inadecuada” o “difícil” por criterios objetivos y reproducibles.
Un hallazgo interesante es que la fuga de la mascarilla no fue un predictor independiente. En otras palabras, una fuga importante no siempre significa una ventilación ineficaz si aún se logra generar un volumen tidal adecuado.
Además, el estudio mostró que la experiencia del anestesiólogo no mejoró el rendimiento del modelo, lo que sugiere que los criterios seleccionados capturan de forma robusta la dificultad real y no solo la percepción del operador.
🫀 Septic Shock Is Not Just About Blood Pressure: It Is About Ventriculo-Arterial Coupling
For years, septic shock resuscitation has focused on restoring MAP, increasing cardiac output, and normalizing lactate.
But what if the real problem is not flow alone?
What if the heart and arterial system are no longer working together?
This is the concept of ventriculo-arterial coupling (VAC): the dynamic interaction between ventricular contractility (Ees) and arterial load (Ea). When coupling is preserved, the cardiovascular system operates efficiently, maximizing stroke work while minimizing myocardial energy expenditure.
Why VAC Matters in Septic Shock
Sepsis causes profound vasoplegia, myocardial depression, and alterations in vascular tone.
As a result, many patients develop ventriculo-arterial uncoupling, where ventricular contractility and arterial load become mismatched. This leads to:
✅ Reduced cardiovascular efficiency
✅ Increased myocardial energetic cost
✅ Impaired tissue perfusion despite apparently adequate cardiac output
✅ Variable responses to fluids, vasopressors, and inotropes
In other words:
Two patients may have the same MAP and cardiac output but completely different cardiovascular efficiency and energetic burden.
The Norepinephrine Paradox
One of the most interesting concepts highlighted by Pinsky and Guarracino is that increasing blood pressure does not always improve cardiovascular performance.
In some septic shock patients with depressed contractility:
🔹 Norepinephrine increases arterial elastance (Ea)
🔹 MAP rises
🔹 Left ventricular afterload increases
🔹 Stroke volume may fall
🔹 VAC worsens
🔹 Cardiac output may remain unchanged or even decrease
The monitor shows a better blood pressure.
The ventricle may actually be working less efficiently.
Why Some Patients Respond and Others Do Not
The review provides a physiological explanation for the heterogeneity we see every day in the ICU.
Patients with preserved contractile reserve may tolerate increased afterload and maintain efficient coupling.
Patients with septic cardiomyopathy may not.
This may explain why identical norepinephrine doses can produce dramatically different hemodynamic responses among seemingly similar septic shock patients.
Beyond Left Ventricular Function
The same principles apply to the right ventricle.
In septic patients with ARDS:
🔹 Pulmonary vascular resistance rises
🔹 RV afterload increases
🔹 RV-pulmonary artery coupling deteriorates
🔹 Venous congestion develops
🔹 Organ perfusion worsens despite acceptable systemic pressures
This reminds us that shock physiology extends far beyond MAP alone.
Clinical Takeaway
Perhaps the next evolution of septic shock management is not simply asking: "Did cardiovascular efficiency improve?"
Reference 📚
Pinsky MR, Guarracino F. Pathophysiological implications of ventriculoarterial coupling in septic shock. Intensive Care Medicine Experimental. 2023;11:87.
https://t.co/3bYkZ1G7wG
PROBESE trial - Más PEEP no es igual a mayor beneficio en pacientes con obesidad..
#AventhoAnestesia#Aventho#SMMCE#SAML
Es verdad que pacientes con estas características clínicas necesitan más PEEP pero, siempre tenemos que balancear los riesgos vs beneficios.
Ninguna intervención es inocua y debemos encontrar el justo balance entre protección pulmonar y estabilidad hemodinámica
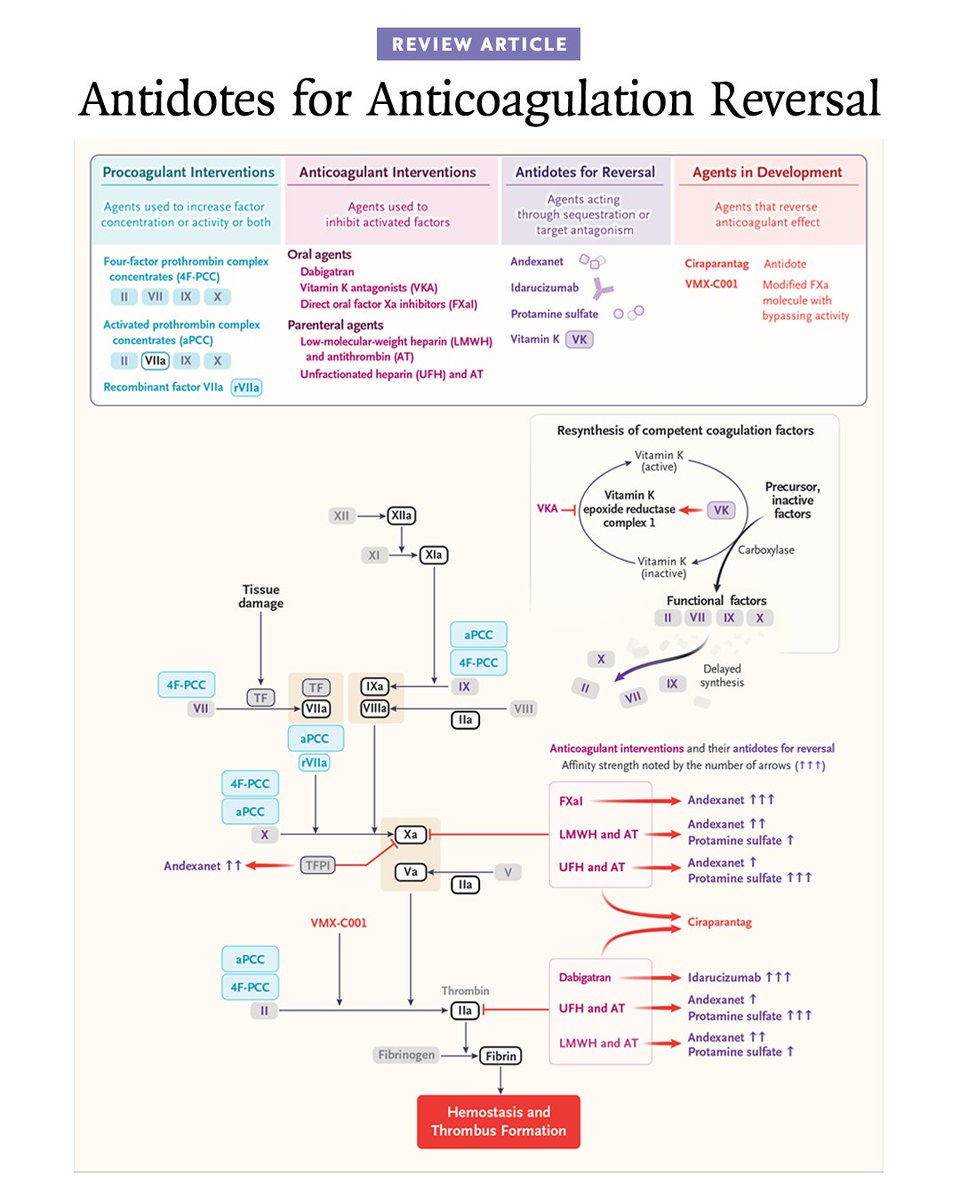
Drs. Bianca Rocca and Hugo ten Cate review current strategies for anticoagulation reversal in major bleeding events or urgent surgery as well as specific antidotes, limits of available evidence, thrombotic risks, unmet therapeutic needs, and ongoing research.
Read the Review Article “Antidotes for Anticoagulation Reversal”: https://t.co/XobqwMebfy
Wondering how you might use this article in practice or teaching? AI Companion can help. Try it with this article.
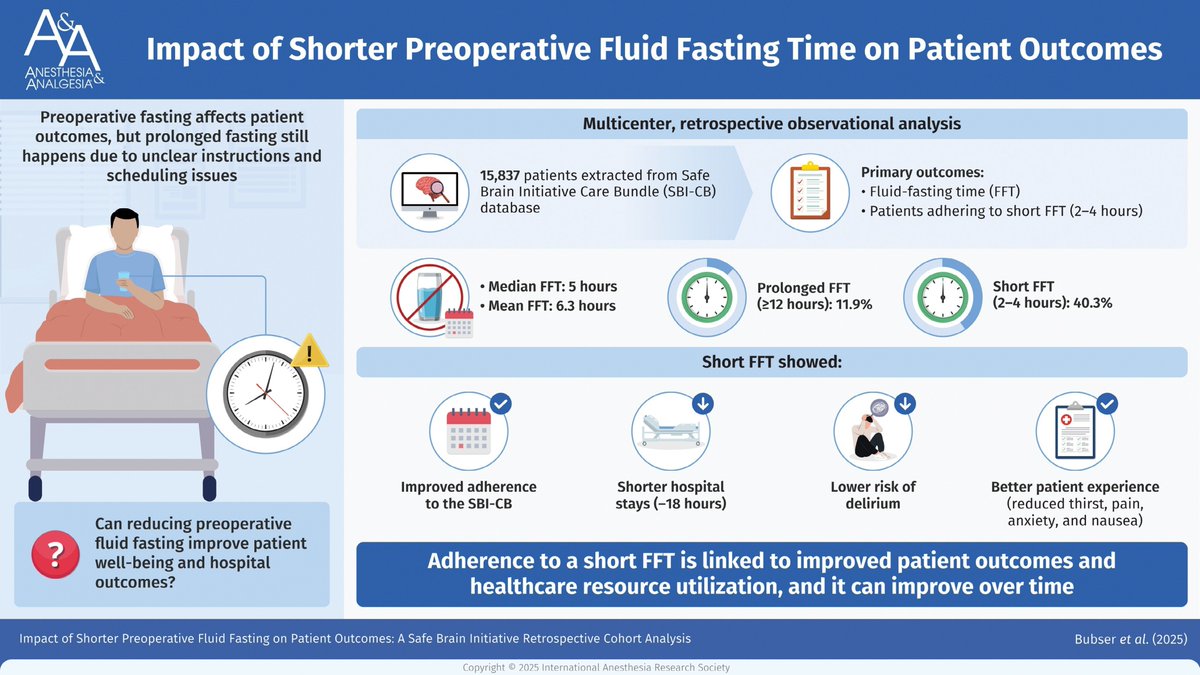
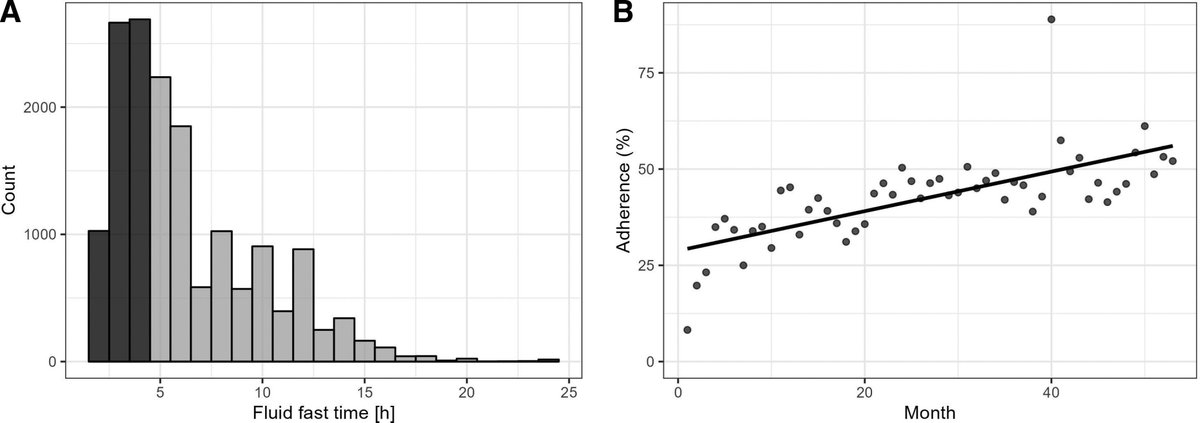
🫗Adherence to a fluid-fasting time of 2 to 4 hours was 40% and could be increased over time with evidence showing a decrease in postoperative delirium in the recovery room, hospital length of stay, and patient-reported outcomes for short (2–4 hours) in comparison with longer times.
https://t.co/nE8PYDz5kS