🎓 REACH: The Research-to-Publication Workshop.
A personalized mentorship for you.
Limited seats: Only 20 seats.
Get your first publication.
For more details, send us a message via WhatsApp:
+201227999117
In our meta-analysis in Cardiovascular Intervention and Therapeutics, we found that among patients with ACS undergoing PCI, stopping aspirin at 3 months ranked highest among all strategies, with no increase in ischemic events.
https://t.co/DQVcS78GbU
@Elsayed_balba3@M0Elgendy
#CardioTwitter #InterventionalCardiology #PCI #ACS
@FCademartiri Congratulations on this important review.
If we have to identify the plaque (we do not know whether there is a plaque), then the question is, "in which diseases?"
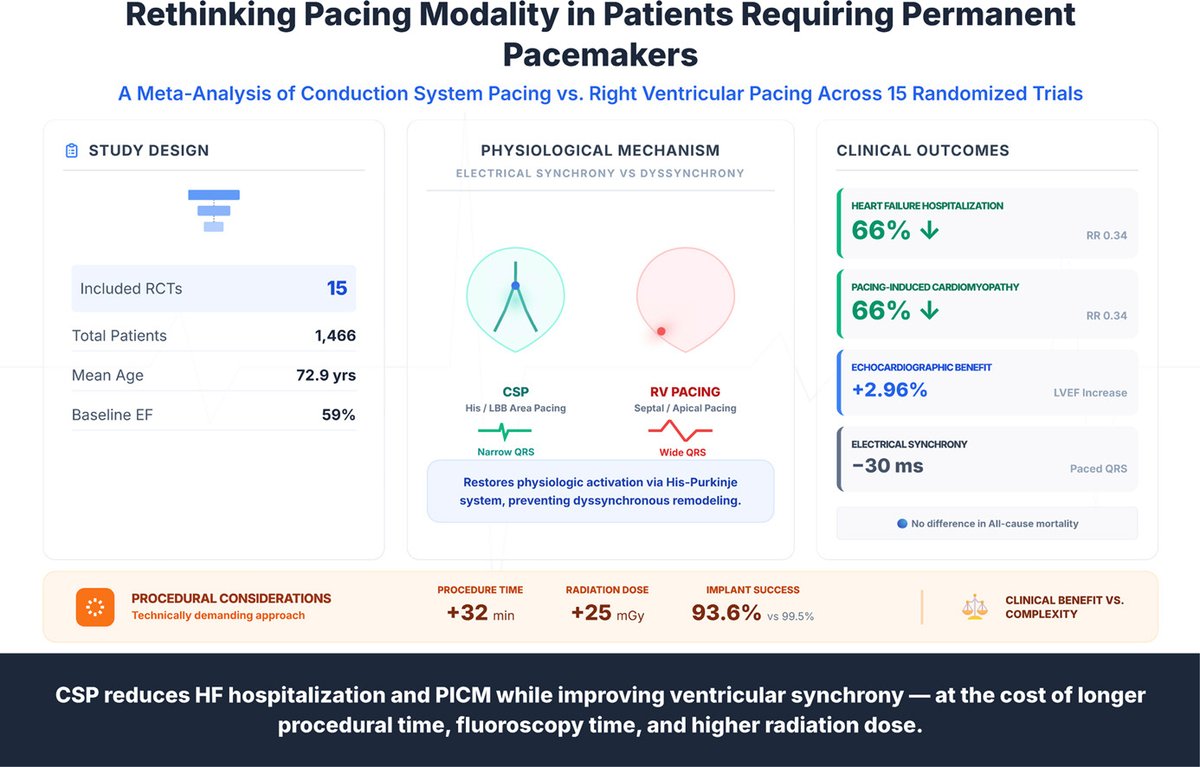
Our meta-analysis suggests that, in patients with preserved/mildly reduced EF and high anticipated ventricular pacing burden, CSP better preserves LV function than RV pacing, reducing PICM and HFH with shorter paced QRS. https://t.co/4OoXR7NtY8
@Teebi_MD@Elsayed_balba3#Epeeps
@drjohnm They have a clear unit of analysis error, see the plot below, pooling the same control 3 times in the same meta overestimates the effect. My question is, if observational studies, from you opinion, are of no value, should we no longer conduct them?
A new EP piece.
🫀 New meta-analysis just dropped in @CJCardiology :
CSP vs RVP in preserved/mildly reduced EF, 15 RCTs, 1,466 pts.
Key findings:
⬇️66% pacing-induced cardiomyopathy (RR 0.34)
⬇️ 66% HF hospitalization (RR 0.34)
⬆️ LVEF by ~3%
⬇️QRS by 30ms
BUT:
⚠️⬆️ +32 min procedure time
⚠️⬇️ Lower implant success (93.6% vs 99.5%)
⚠️⬆️ Higher radiation dose
⛔️No mortality difference.
Bottom line: CSP is a physiologic pacing strategy that protects the LV, but comes at a procedural cost. Worth it when a high RV burden is expected.
@hakeemshubietah, @mohamadsaad_R, @AmeerAwashra, @QasemWsalah, @M0Elgendy, @emara991, @ElbataaMD, @MRuzieh, @DrMarwanRefaat@Teebi_MD
#EPeeps #Cardiology #CSP #Pacing #HFpEF #PhysiologicPacing #LBBAP
🧵 A thought that keeps me up at night:
We anticoagulate AF patients to prevent stroke — but do we ever pause to ask: how many strokes are actually caused by AF?
Evidence says ~20–25% of ischemic strokes are attributed to AF.
(NIH/PMC; ESC; NEJM ELAN Trial 2023)
That means 75–80% of strokes happen for OTHER reasons, yet AF gets much of our preventive focus.
And here's the kicker: ~51% of AF patients eligible for anticoagulation who suffered a stroke weren't even on appropriate therapy beforehand.
So are we treating the rhythm… or preventing the real culprit?
The gap between guideline adherence and real-world practice is where strokes happen. 🔍
#Cardiology #Neurology #AtrialFibrillation #StrokePrevention #MedTwitter
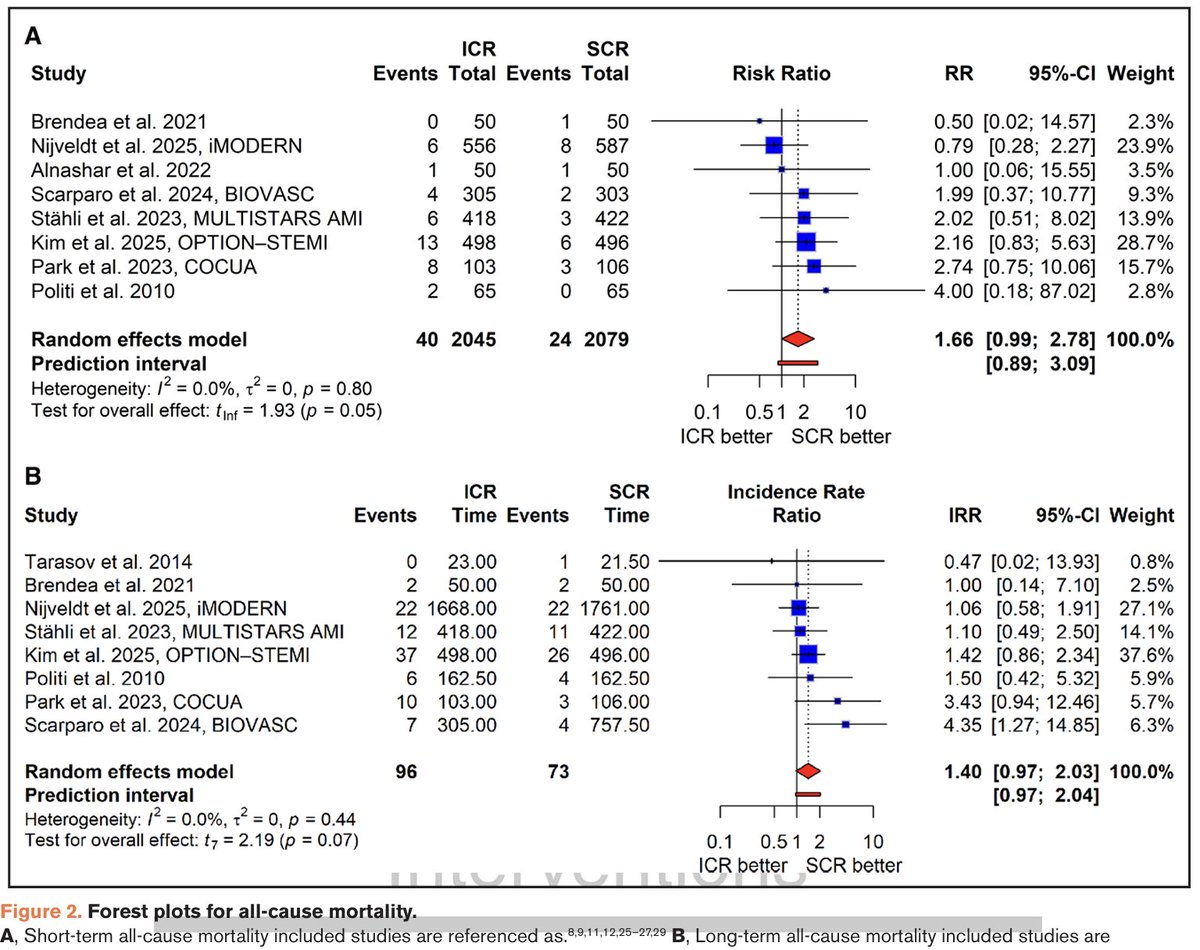
Complete revasc (CR) in pts with non-shock STEMI and multivessel ds. reduces MACE. But is the best timing for non-culprit lsn PCI immediate (during primary PCI) or staged? Our new meta-analysis publ in Circ CV Interv suggests immediate CR may increase mortality, same as in shock.
Sleep timing irregularity in midlife: association with incident major adverse cardiac events and cardiovascular disease mortality over a 10-year follow-up
🫀Individuals with irregular bedtimes had a 2-fold higher risk of MACEs compared to those with regular bedtimes
Irregular sleep midpoints? Also a 2-fold higher risk
https://t.co/1HzYQdywMb
Impact of coronary artery calcium scores on cardiovascular risk and preventive therapies: A systematic review and meta-analysis
@reverohealth @shashiiyengar @Mangan150 https://t.co/p7R1CUaw5i
On that note: The lab is hiring a postgrad researcher to work with both Dr. Ferguson and Dr. Jennifer Richeson starting this summer.
Details below... Come join a new lab with me🤭🤝
We welcome applications for our post-doctoral fellowship in trauma research
Fully funded, 1 +/- 1 year duration, focus on healthcare resiliency
Expertise in large database analyses and R required
https://t.co/9LYYieSYOp