EM pharmacy, healthcare simulation, toxicology, micro dose pressors safety, EM quality and safety, CritCare in ED, harm reduction. Animal lover. Views are mine
Would you consider yourself a resuscitation expert? Comment below how you’d grade your skills from 1-10.
Regardless of where you land, Swami and Scott will make sure this segment has something for you to take away to your practice, and you are going to want to tune in to hear it.
They will be discussing
👍 The Good: Higher first-shock energy settings (≥200 J) are preferable to lower energy.
👎 The Bad: Guidelines still say to continue giving Epi every 3 to 5 minutes. There is no definitive evidence of improved neurologic outcomes, and outcomes may be worse in shockable rhythm states.
❌ The Ugly: International Liaison Committee on Resuscitation (ILCOR) states that dual sequential external defibrillation (DSED) may be performed for shockable rhythms.
One important thing to note: The ACLS guidelines were made for all-comers in medicine and, therefore, should be approached with understanding that your expertise as a resuscitationist may go beyond ACLS.
#EMRAP #EM #EmergencyMedicine #ACLSGuidelines #AHAGuidelines #resuscitation
Rocuronium has a dose-dependent onset AND duration. While it is appropriate to give a dose at the higher end of the range for faster onset (up to 1.6 mg/kg IBW) in the setting of a crash airway, the practice of “blanket dosing” 100 mg for all patients should be reconsidered.
Large doses cause an extended duration of action and greatly increase risk of awareness with paralysis. If you haven’t read the ED-AWARENESS Study, please do so.
Rocuronium should be dosed at 1 mg/kg IBW (roc is hydrophilic) with the rare crash airway exception.
@PharmacyAcute This is excellent! Consider adding epinephrine potentially causing lactic acid elevation by increasing glycolysis and anaerobic metabolism. Can cloud the picture in post-arrest resuscitation!
The 2025 AHA/ACC Hypertension Guidelines are out, and the changes are significant. Here are the key takeaways for pharmacists & clinicians:
"Hypertensive Urgency" is now "Severe Hypertension" for BP >180/120 w/o target organ damage.
Move away from IV meds for asymptomatic severe HTN. Oral initiation is key.
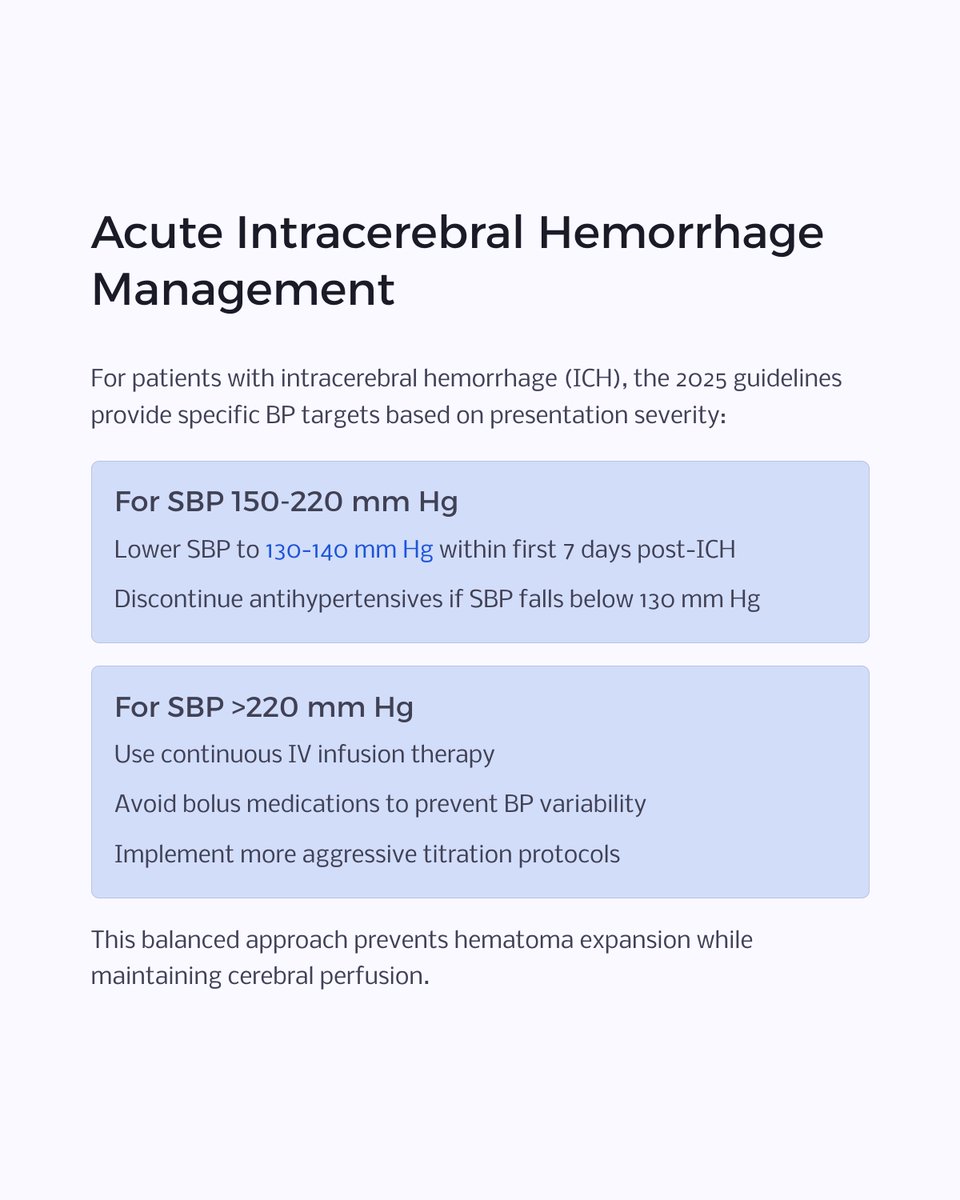
New, specific BP targets for ICH & post-reperfusion ischemic stroke.
The PREVENT risk calculator is in, setting new thresholds (≥7.5% risk) for starting meds at BP ≥130/80.
Swipe through the carousel for a full visual breakdown of these practice-changing updates!
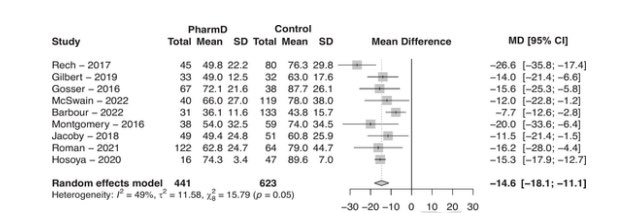
💡 Need one more reason to love your friendly EM pharmacist? Check out this @EMPHARM_NET SR/MA:
⏰ EMP presence was associated with reduced mean DTN time by 14.6 minutes (95 % CI -18.1, −11.1 min)
Time for @American_Stroke@American_Heart to take notice?
It’s time, once again, to enter the realm of TXA (tranexamic acid) in trauma! Recent updates mean we can often give this powerhouse with a quick 1-2 gram IV push, instead of a long, resource-intensive, 8-hour drip. Talk about efficiency!
Plus, at typical trauma doses, you don't need to worry about the "prothrombotic" villain—those studies used a whopping 4g, way more than our heroic doses! So whether you're following the Tactical Combat Casualty Care's 2g guidance or NAESP's 1-2g, remember: TXA is on your side, helping to keep things clotted in all the right places!
#TraumaTalk #TXAFunFacts #emergencymedicine #trauma #EMRAP
Emergency medicine and critical care pharmacists play an integral role in trauma resuscitation/MTP. Our article sums up key information in the management of this patient population. @ASHPOfficial@accpemedprn@SCCM_CPP@EMpharmacists@SAEM_AEMP
https://t.co/VkbizOsu1G
Check out our new segment on anti-amyloid mABs to learn why you need to be aware of these meds in the ED 👇
🧠 ADEs called ARIAs are non-specific, typically require MRI & can mimic stroke
⛔ Concomitant thrombolytics/anticoagulants are contraindicated
https://t.co/WVOcuG2JqO
New SRMA in-press with 6 studies comparing re-arrest rates post-ROSC btwn epi and norepi gtts with NE showing lower re-arrest rates and a non-significant increase is survival to discharge
Should likely be doing NE gtts in most everyone post-ROSC at this point