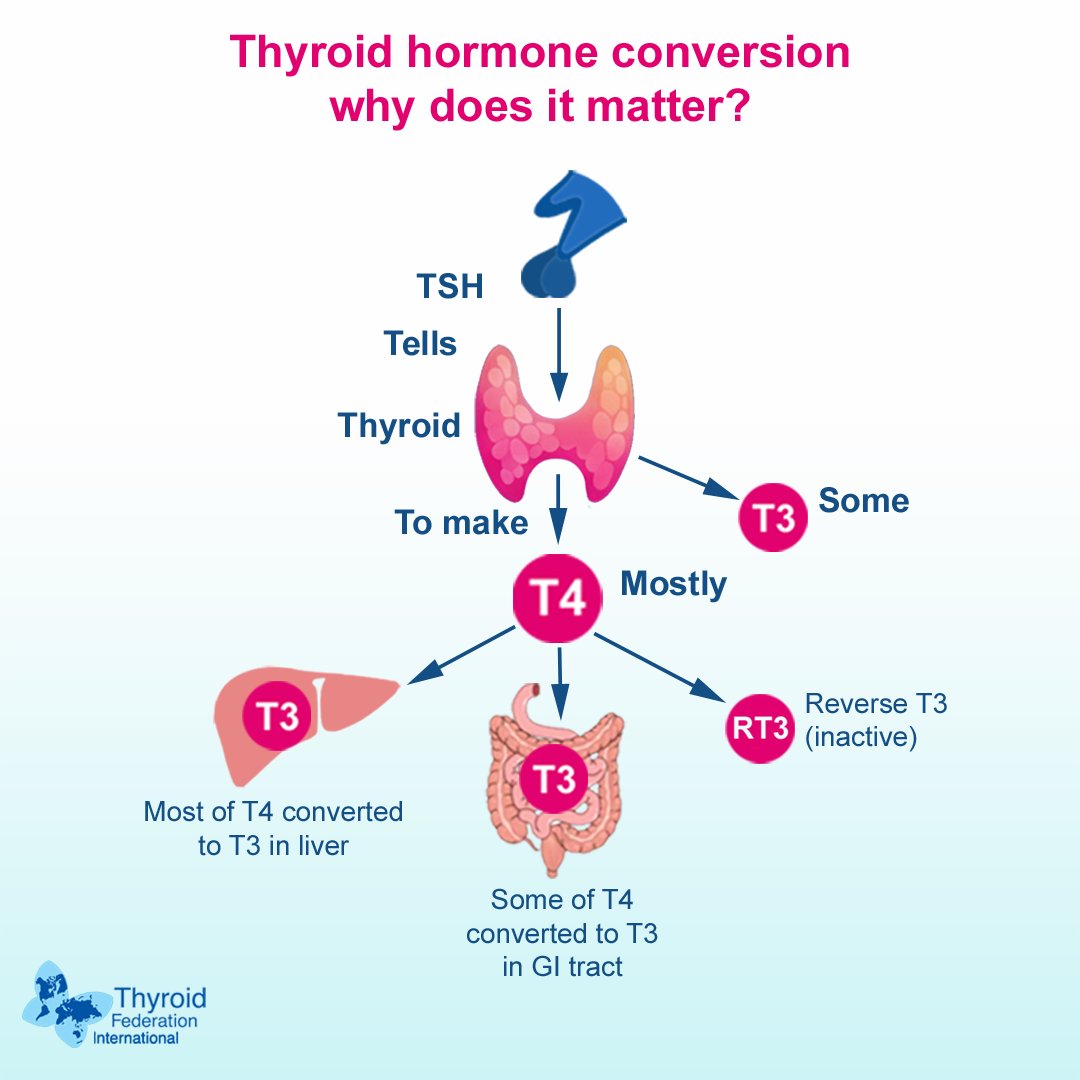
Thyroid hormone conversion is the peripheral process where T4 is converted into T3. To ensure optimal treatment of hypothyroidism, it is important to understand thyroid physiology and thoroughly evaluate thyroid dysfunction.
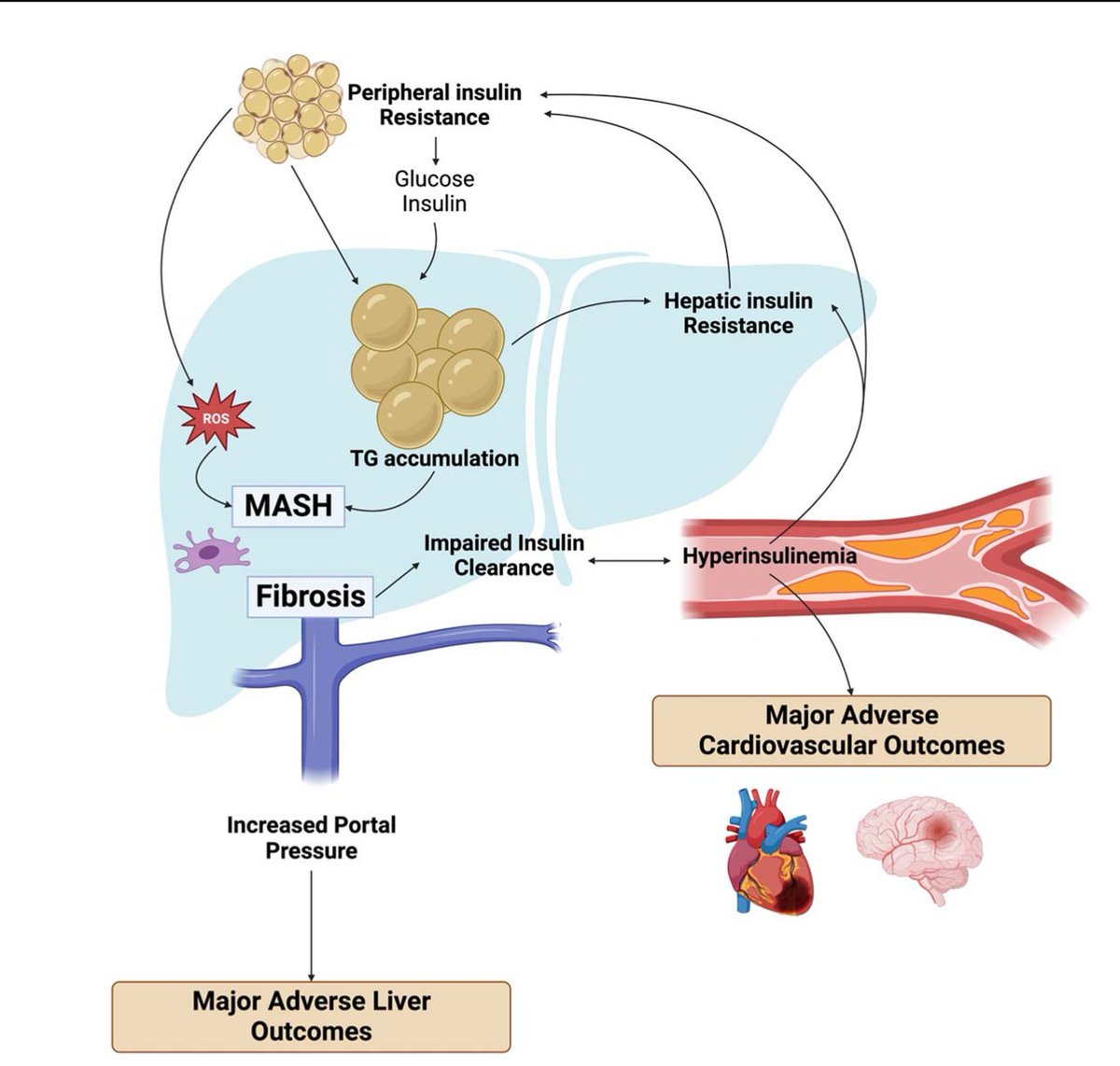
Liver fibrosis + hyperinsulinemia are central drivers of bad outcomes in MASLD/MASH. The MASLD pathway → liver fibrosis + impaired hepatic insulin clearance → worsening insulin resistance + hyperinsulinemia (an independent predictor of MACE). Liver fibrosis also ↑ portal pressure, predisposing to major adverse liver outcomes.
https://t.co/sFgRlpXPZo
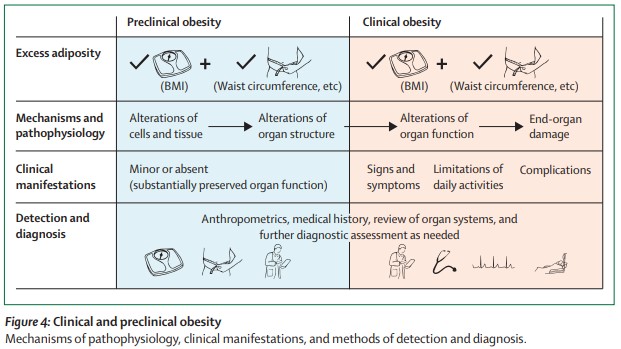
Our #MostRead article in 2025:
Definition and diagnostic criteria of #clinical#obesity https://t.co/cM8pyJ2UG9
#FREE to read with registration (also FREE)
💊🫀 Lipidology in 2025: from “lower LDL” to precision prevention
This expert discussion in the Journal of Clinical Lipidology (2025) offers a rare, insider view on how lipid-lowering drugs are actually conceived, developed, and translated into practice—and where the field is heading next .
🧠 A mature field facing new challenges
LDL-C remains a causal driver of ASCVD, but lipidology has moved far beyond statin monotherapy. The discussion highlights a central tension: we have more effective drugs than ever, yet treatment inertia remains profound, with many high-risk patients still undertreated.
🔬 How new lipid drugs are born
Successful development now hinges on:
Genetic validation (Mendelian randomization) to de-risk targets
Surrogate endpoints with regulatory credibility (LDL-C remains king)
Cost-effectiveness, safety, and tolerability, often more important for uptake than maximal efficacy
PCSK9 inhibitors are used as a cautionary tale: biologically sound, outcome-proven—but initially underutilized due to pricing, complexity, and unrealistic expectations.
💊 What’s coming next?
The future is multi-target:
Lp(a) therapies are poised to reshape prevention 🧬
CETP inhibition (e.g. obicetrapib) aims for “LDL-lowering plus” effects, including Lp(a) reduction and metabolic benefits
Remnant cholesterol, ApoC3, and inflammation (IL-6, NLRP3) emerge as key residual-risk targets
Imaging endpoints (non-calcified plaque volume) may help de-risk and accelerate drug development
⏳ The most important message
Prevention must start earlier and longer. Modest LDL reductions in low-risk individuals may yield greater lifetime benefit than aggressive treatment late in disease.
🔮 Bottom line
We already have the tools to prevent ASCVD. The real challenge is using them earlier, smarter, and together—moving lipidology from reactive treatment to precision cardiovascular prevention 🚀
👉Pharmacotherapy development and trends in lipidology: An expert discussion
☝️Key takeaways
1️⃣ ASCVD prevention remains lipid-centric: Lowering atherogenic lipoproteins—especially LDL-C—continues to be the cornerstone of cardiovascular risk reduction, but it is no longer enough on its own.
2️⃣ “Lower for longer” matters: Earlier intervention across the life course yields greater relative risk reduction than late treatment in advanced disease. Biology is stubborn; it remembers cumulative exposure.
3️⃣ Beyond LDL-C: Emerging targets include lipoprotein(a), remnant cholesterol, ApoC-III, and vascular inflammation—each addressing residual cardiovascular risk left behind by LDL-C lowering alone.
4️⃣ Lp(a) is moving center stage: High patient demand, strong genetic causality, and multiple therapies in development are likely to transform screening and management strategies.
5️⃣ Treatment inertia is the real enemy: Underutilization of proven therapies (e.g., statins, PCSK9 inhibitors) reflects gaps in goal-oriented care, cost concerns, and patient mistrust—safety and simplicity drive adherence more than marginal efficacy gains.
6️⃣ Oral, well-tolerated therapies are game-changers: Ease of use and safety may determine real-world impact more than mechanism novelty.
7️⃣ Imaging and surrogate endpoints: Non-calcified plaque and other imaging biomarkers may help de-risk development and accelerate access—outcomes trials alone are becoming unsustainably large and slow.
8️⃣ Cardiometabolic convergence: Lipid management, obesity treatment, diabetes prevention, and inflammation control are synergistic—not competing—strategies.
9️⃣ The future vision: Aggressive LDL-C lowering plus early, comprehensive control of lipids, inflammation, and metabolic risk—started before disease declares itself. Old-school prevention, backed by modern tools.
🔓Open Access https://t.co/HA8Y4uNdqc
@LipidJournal@nationallipid@CBallantyneMD@society_eas
"Mancuernas"
Porque está es la forma correcta de hacer un entrenamiento completo con mancuernas. Y vos seguro lo estabas haciendo como el orto en el gimnasio, empezá a hacerlo bien, pedazo de pelotudo.
🙌We are pleased to share our latest publication:
“Inhibition of ANGPTL3 as a target for managing hypertriglyceridemia”
recently published in Current Opinion in Endocrinology, Diabetes and Obesity.
👉Scope: Comprehensive review of ANGPTL3 inhibition as a therapeutic strategy to reduce triglyceride-rich lipoproteins and residual cardiovascular risk
👉Therapeutic approaches discussed:
– Monoclonal antibodies (e.g., evinacumab)
– RNA-based therapies (ASOs and siRNA: vupanorsen, zodasiran, solbinsiran)
– Emerging gene-editing strategies (CRISPR/base editing)
👉Key message: Targeting ANGPTL3 provides robust reductions in triglycerides, apoB-containing lipoproteins, and non-HDL cholesterol, independently of the LDL receptor
👉Clinical relevance: Positions ANGPTL3 inhibition as a next-generation approach for managing mixed dyslipidemia and lipid-related residual risk beyond LDL-C
🔗 https://t.co/G2s4HB4RRi
@society_eas@lschreier1@natinardelli_@CO_EndoDiabetes
🚨 Si tu Gmail se ha quedado sin espacio, esto te va a salvar.
Cuando alcanzas el límite, Gmail deja de funcionar con normalidad.
Te explico cómo liberar espacio paso a paso 👇