@murphy_lzy@Hapa_EP@sachinjv@forkknifecab_EP@JeffZhanghk2017@Mya49099911@AbbottCardio Choice of site to terminate this is pretty interesting. If ablating where indicated this should be near bachmanns. What are the possible consequences and how would you validate the ablation lesion? Curious to see post ablation map and the p wave morphology afterwards
@murphy_lzy@Hapa_EP@forkknifecab_EP@sachinjv@JeffZhanghk2017@Mya49099911 I think I remember this case. It’s a nice case showing a lot of passive activation. I confess I don’t usually ablate potential circuits (exception being CTI) but seeing the left map I think I might try hard to induce a flutter and if it’s inducible, then choose to go after it.
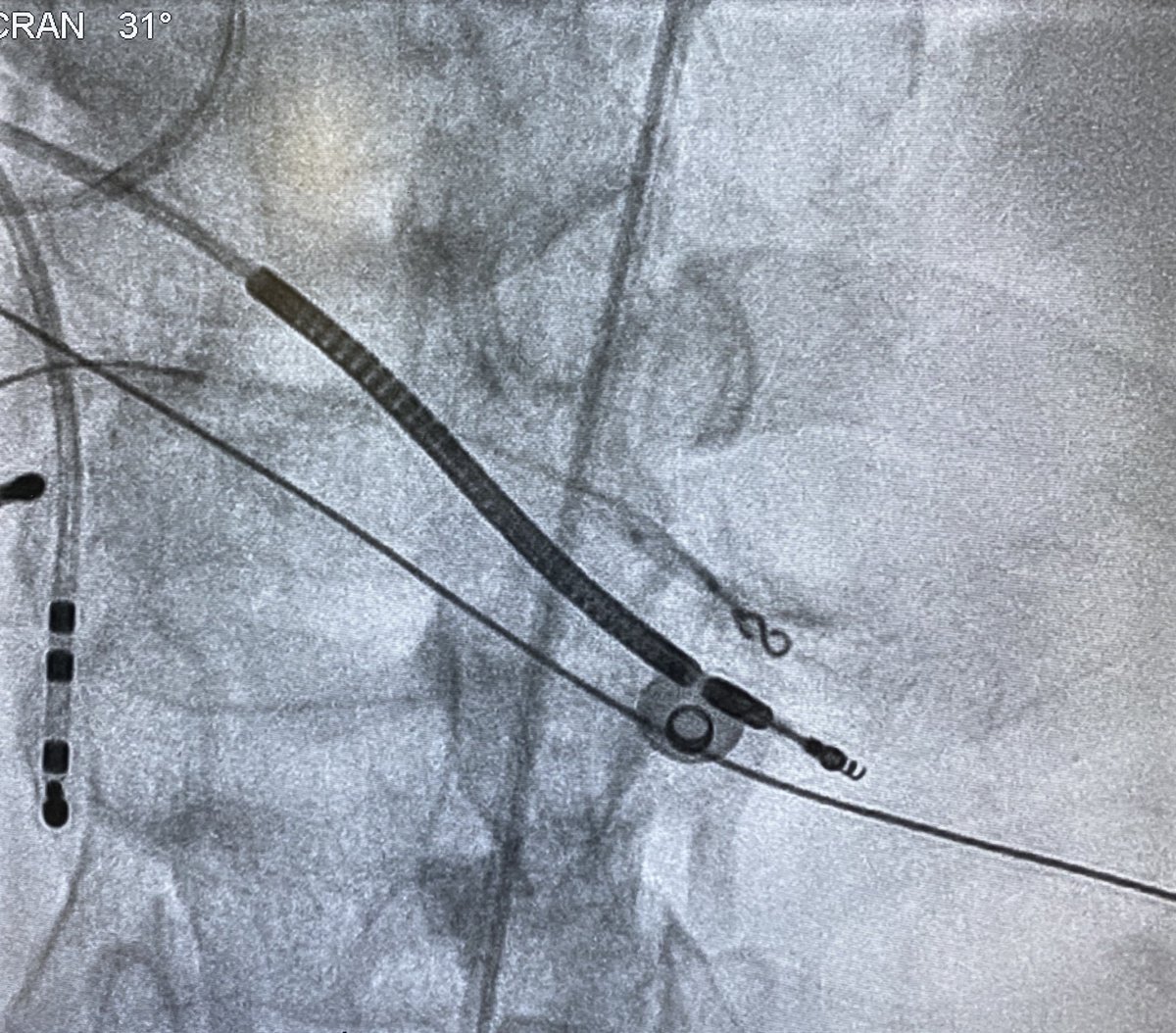
@jeffrey_vinocur@murphy_lzy@rabinkova Actually for this case although we had used a Biotronik vision wire for the initial mapping, we changed to a PCI wire and used a micro catheter to insulate the prox portion. Indifferent electrode is in IVC. You can see good signals with it (white trace on pic).
@rabinkova It is a special guidewire with connection cable provided by Biotronik, but I am thinking normal guidewire plus alligator clip should work as well. The signals were unipolar, there was an indifferent electrode in IVC.
@murphy_lzy@sachinjv@Hapa_EP@JeffZhanghk2017@Mya49099911@AbbottCardio This was the septal VT from today, Murphy. No maps since we’d mapped it previously. First pic shows termination with cold saline in RPDA. Wire mapping shows concealed entrainment with TCL-PPI of zero. Coiling+gel foam in distal RPDA renders VT uninducible
Activation properties during sinus rhythm may be helpful for differentiating myocardial infarctions that are vulnerable for VT from those less vulnerable for VT #AHAjournals
https://t.co/yCKiGWnrq0
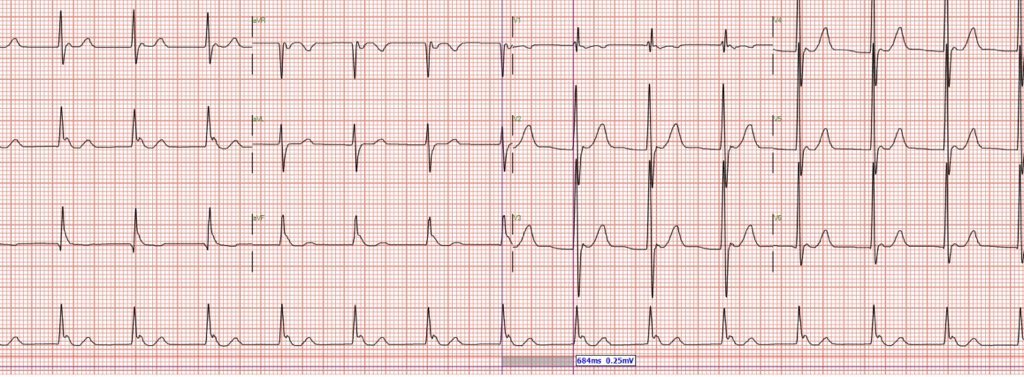
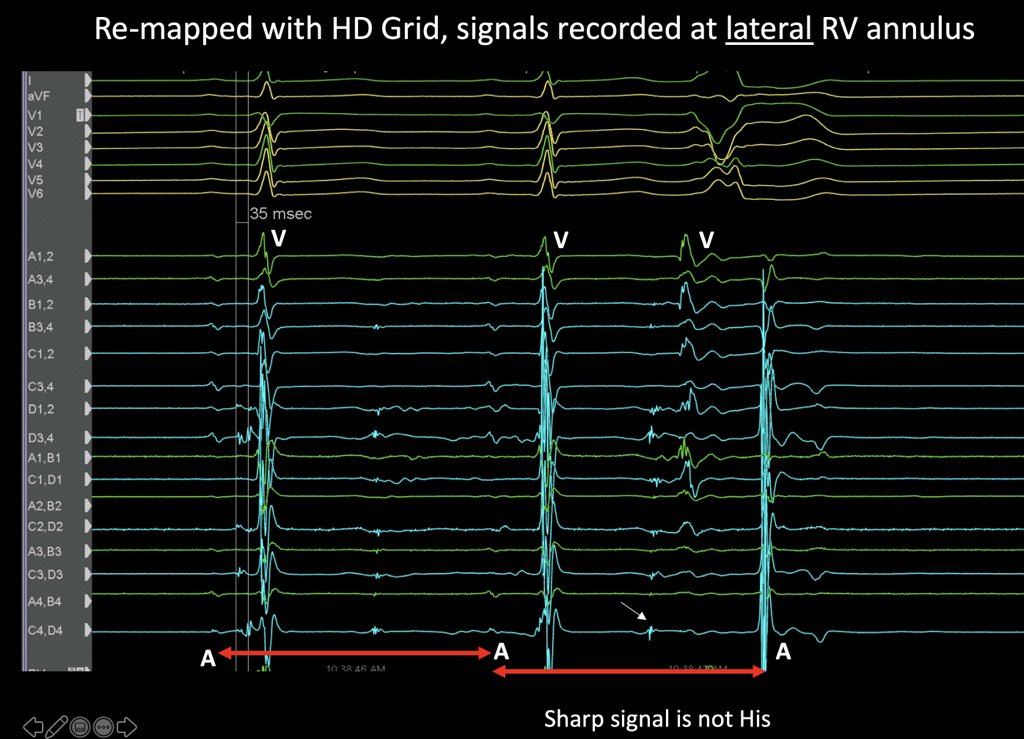
@murphy_lzy@ericlim1975@Hapa_EP@JeffZhanghk2017@Mya49099911@AbbottCardio Pretty interesting case. PVC somewhat pleomorphic and a little challenging to localise from the 12 lead. Very late potentials in SR which become precocious during PVC - sharp, almost Purkinje-like except I recorded it at lateral TV annulus. RF induced VT immediately.
@murphy_lzy@ericlim1975@Hapa_EP@JeffZhanghk2017@Mya49099911@AbbottCardio 4/ So despite the timing across the CTI you showed of 205ms, decreasing laterally, CTI is not actually blocked. If timing was taken more towards the IVC end, it would be a LOT shorter. Without an activation map and/or careful measurements it would be quite easy to make a mistake
@murphy_lzy@ericlim1975@Hapa_EP@JeffZhanghk2017@Mya49099911@AbbottCardio 2/ But the activation map shows that there is an unusual pattern of activation where there is a gap at the IVC end of the CTI, *plus* a line of block causing activation to sweep laterally before turning in laterally. Hence the impression of block which is false.
@murphy_lzy@ericlim1975@Hapa_EP@JeffZhanghk2017@Mya49099911@AbbottCardio Would be good to have little more explanation, Murphy. RV pace map doesn’t just show an isochronally crowded / deceleration zone but there’s a putative channel there. That’s why Grid was placed there and extras used to stim+ induce VT with immediate mapping of diastole.