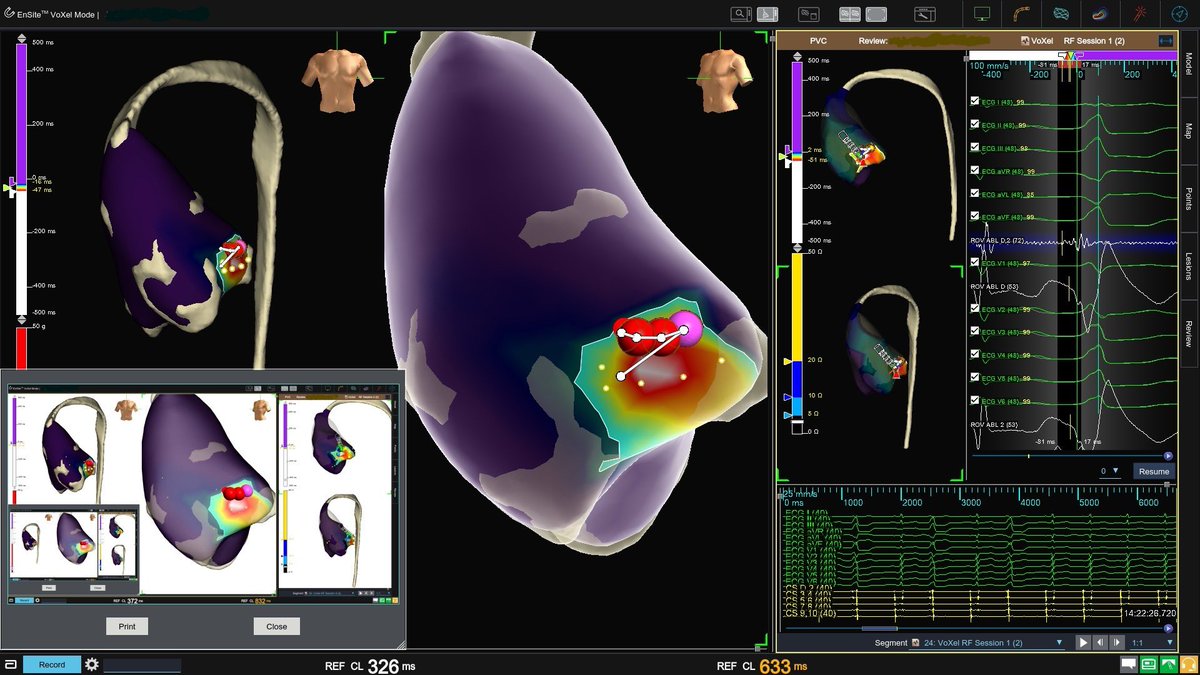
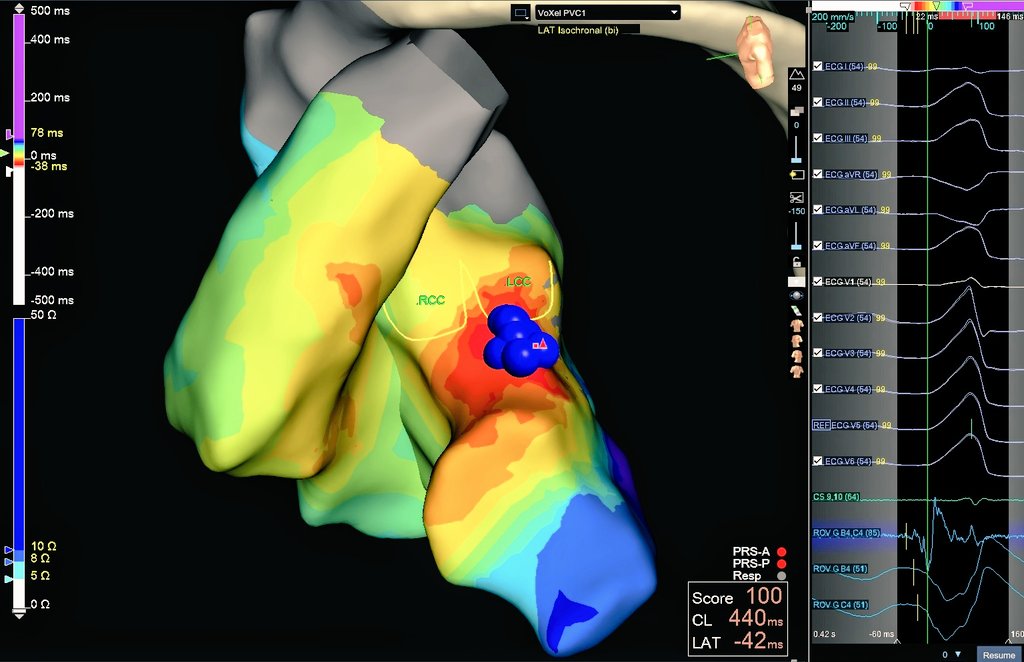
Premature ventricular complexes with a QRS morphology almost identical to the sinus rhythm was caused by a His-LBB twig that could be successfully ablated in or underneath the right coronary cusp without injury to the conduction system. https://t.co/Xirmhr67Ri #JACCCEP
Volt released some pretty impressive 12 month data with over 80% success in paroxysmals and excellent persistent AF results. Read the simultaneous publication! https://t.co/rXBZzjlPj1
First-in-Nation: Integrating ViewFlex X SE ICE with VOLT PFA
This week started with a meaningful milestone at St. Bernards Healthcare (Jonesboro, AR) — first-in-nation combining Abbott’s ViewFlex X Sensor Enabled ICE with the VOLT PFA platform.
This builds on our prior experience with:
• FIH clinical trial use of ViewFlex X SE
• Post-FDA VOLT PFA cases as part of the VOLT LMR
What stood out was how well imaging + mapping + energy delivery functioned as one ecosystem in a zero fluoroscopy / zero contrast workflow .
Key takeaways
🔹 ICE integrated into EnSite X for real-time anatomic confirmation during PFA
🔹 Safe ICE-in-LA workflow and transseptal planning that reduced unnecessary manipulation in small LA anatomy. Integration helped support transseptal decision-making up front—optimizing trajectory and reducing unnecessary catheter manipulation in small LA anatomy.
🔹 Quick LA shell creation to confirm ridge/posterior wall/carina geometry early
🔹 Small atria lesion strategy: integration helped us decide tighter antral lesions vs intentionally addressing a posterior “critical isthmus” when the posterior corridor was inherently narrow
🔹 During VOLT delivery: very low microbubble visualization on ICE and no clinical hemolysis observed
VOLT workflow highlights: single-catheter mapping/pacing/ablation, impedance-based contact visualization, balloon-in-basket (8 splines), selective electrode delivery; PVI ± PVI+ as clinically indicated (GA used).
Grateful for the St. Bernards EP Lab team and the Abbott clinical support team.
#ViewFlexXSE #VOLTPFA #FirstInNation #ICE #EnSiteX #ZeroFluoro #ZeroContrast #EPWorkflow #Innovation #epeeps
@StBernards | @ARGJonesboro I @AbbottNews I @AbbottCardio
Happy to share!We Just completed our first Chagas VT ablation integrating anatomy & EAM @inheartmedical
🔹Precise visualization of phrenic nerves & coronary vessels🔹Detailed scar heterogeneity/transmurality🔹 LV wall thickness & maps.Massive leap for complex CMP #ablateVT
Starting the year with a recap on a recent challenging VT case at @mhshospital@Mapbastian@JC_EPMaps@mike_lean@joel_chic
A 3rd time redo in a non-ischemic VT patient.
Success in these cases requires the use of advanced techniques - however, advanced techniques do not mean unsafe procedures.
Some specific workflow highlights that led to a successful bipolar case without complications and 0 clinical VT on follow-up:
- Meticulous mapping was performed to fully understand each VT before delivering energy.
- Reentrant VTs are inherently 3D in nature, often revealing only a portion of the channel in the chamber mapped (in this case, only the exit for each VT).
- Entrainment at the presumed VT exit confirmed what the map suggested.
- Remote entrainment from the RV was helpful to confirm diastolic signals on mapping catheter were within circuit.
#AblateVT #EPpeeps #WIC #WomenInEP
Meet Volt™ PFA System, now FDA-approved: The latest-generation tech to treat AFib. Shorter procedures, smoother recovery, and better long-term results — Volt makes it possible.
More 👉 https://t.co/HFqz3gJKb2
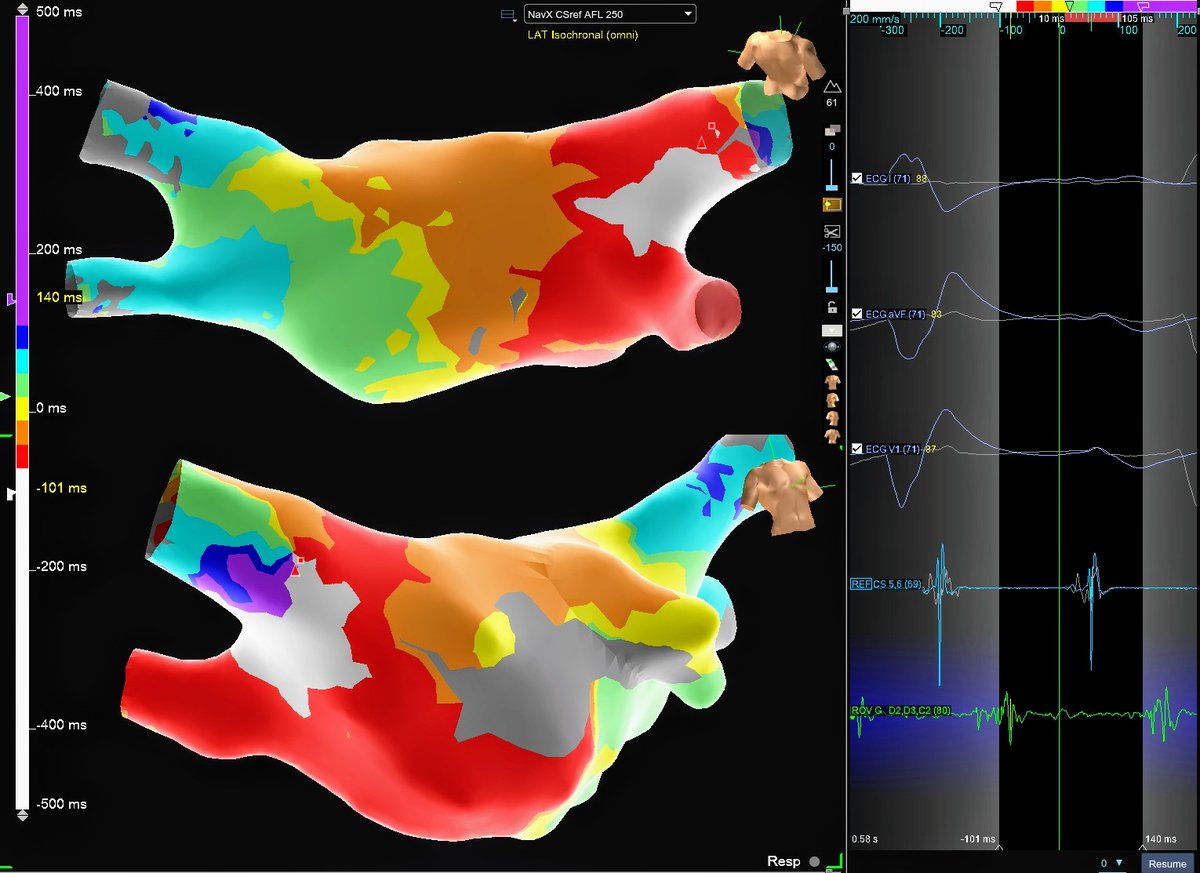
Here are LAT & voltage maps in VT with each detection algorithm.
I do agree about the need to appropriately delineate LOB/split signals. With that, we have actually found NF to work great in objectively annotating those signals. However to your point, it does come down to physician preference and many prefer to see the full circuit.
With that, in some cases we will switch to FD to force annotation of signals that are presumably deeper in the myocardium and not detected by OT NF. Either way, it is helpful to TurboMap and have both maps in a case.
Some post-case learning with @danealson (Dr. Neal Bhatia) and @_shannonmillard: following an ischemic VT case, together we compared how the clinical VT circuit presented when mapped with the First Deflection algorithm versus EnSite™ OT Near Field.
What we found brings up an interesting question. Is it better to….
- Force the system to visualize the full circuit with First Deflection, or
- Illustrate the potential midmyocardial bridges and touchdown points with OT NF?
While there may not be a "correct" answer, we think there is value in appreciating both pieces of information. And if nothing else, it makes for a fun discussion with talented colleagues like Dr. Bhatia and Shannon.
What actually "looks good" on ICE:
#ViewFlex Left Atrial imaging @EPS_PDX
Training @MRazminia
Sponsored @AbbottCardio
Complemented #EnSiteX PFA Visualization & Contact Index software.
A post PFA induced tachycardia, entrained at downstream electrogram, with long upstream capture (>75%, seen on splines) confirmed #Reentrant mechanism & circuit participation.
Rare RA septal flutter on a patient with prior mitral valve surgery as well as PFA PVI, SVC isolation, intercaval line for lateral wall atriotomy scar flutter, and RF CTI line. Where would you burn? Or would you go transseptal to map LA? @narrowQRS@Maeskander@jeffrey_vinocur
A frequent PVC, ablated at interleaflet triangle, an anatomic gift.
12 lead ECG morphology consistent with successful site.
ILT catheter navigation & contact enhanced with Intracardiac Echo.
@georgecrowell@AbbottCardio#TactiFlex#ViewFlex
Full lesion set with consolidation rosette 🏵️. The PVC never came back after the first lesion, consolidation RF, and a 20-minute waiting period. Should we give isuprel even though the patient was in bigeminy up until RF? We did not, but now I am wondering if we should have.