EP at National Heart Center Singapore. Views expressed here are my own and don’t represent the institution. Interested in mapping and conduction system pacing.
@MRazminia Thanks. I guess you probably place ICE through the same TSP as the Faradrive? Although I have done this also, I do have concerns aboutiatrogenic ASDs when placing both a 10Fr ICE plus the Faradrive (ID 13Fr) together through the same puncture. Is this a concern for you?
@MRazminia Do you do this through a single transseptal puncture site? If so do you worry about the size of the hole needed to accommodate both a Faradrive and ICE catheter?
@James_Elliott01@finnakerstrom@enes_elvin@riley_guntrip@chris_monkhouse I agree LOT-CRT has a lot of added baggage and I’ve tended to avoid them after going through a stretch of time trying them. At the end of this case, my regret is that I did not test adequately the LBB-CRT configuration and kept to that. Perhaps others can learn from my mistake.
@curilakarol@finnakerstrom@James_Elliott01@enes_elvin@riley_guntrip@chris_monkhouse Retrospectively, I would have tested impact of optimizing AV delay after getting the LBB lead in, since LBBP-CRT with RBB fusion gave such a nice result (without CS lead). But like others in this thread, I was convinced I needed a LOT-CRT. Turned out I was wrong - lesson learned.
@JoelSimonEP@finnakerstrom@James_Elliott01@enes_elvin@riley_guntrip@chris_monkhouse Hi, yes there’s a ICD lead but it’s a DF1 lead. Defib part is connected to DF1 port for shocking but the LBB lead is connected to the pace-sense port. So pacing occurs via the LBB lead and the RV defib lead can shock but can’t pace. Allows connection to a standard DF1 CRTD PG.
6/ Actually, with CSP lead only+RBB fusion, we got a QRS almost as good. Previous morphology slightly nicer I think but is this worth the complexity of a LOT-CRT cf. LBB-CRT? (Would be a no from me). Overall, I thought this was an interesting case worth sharing with #Epeeps.
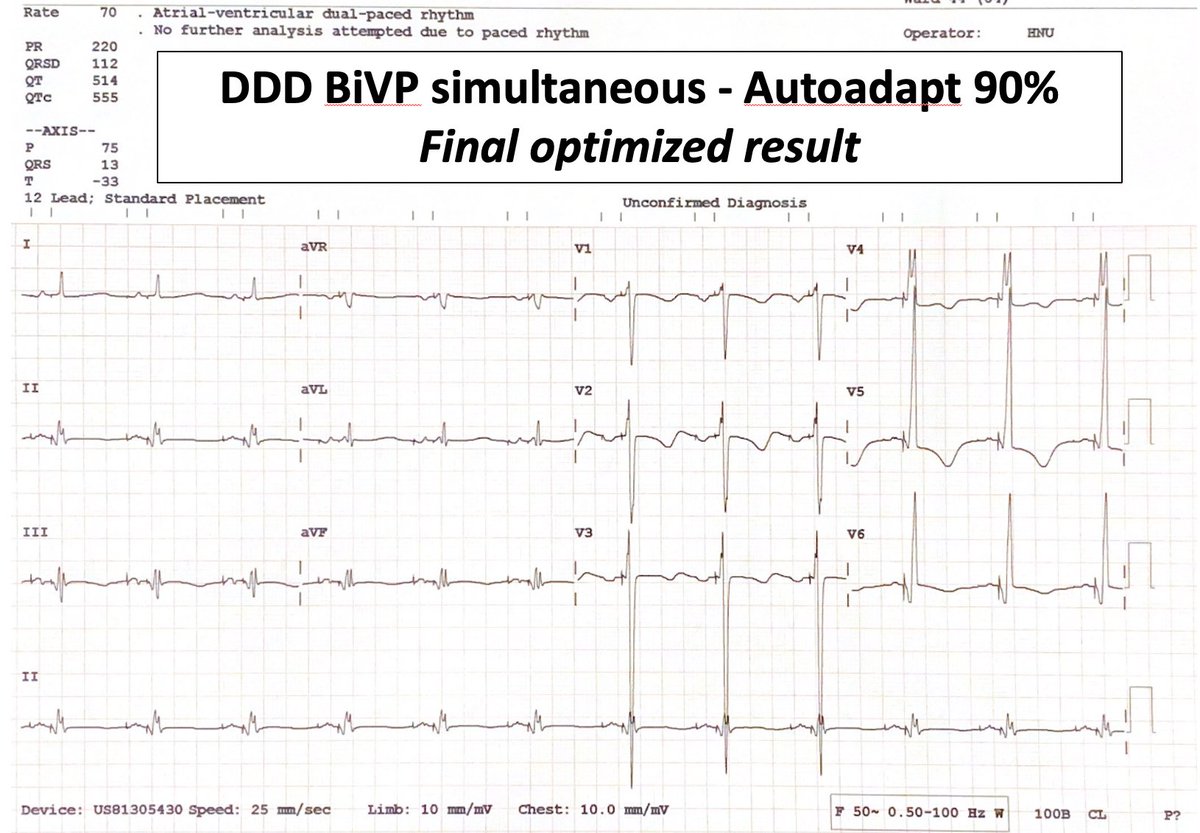
5/ This was the final optimised result with both LBB and CS lead pacing, and after adjusting VV plus the AV delay (which Biotronik allows via the autoAdapt %). It does look very good, with a QRS of around 110ms. But what if I had only used a CSP lead (or CS lead)?