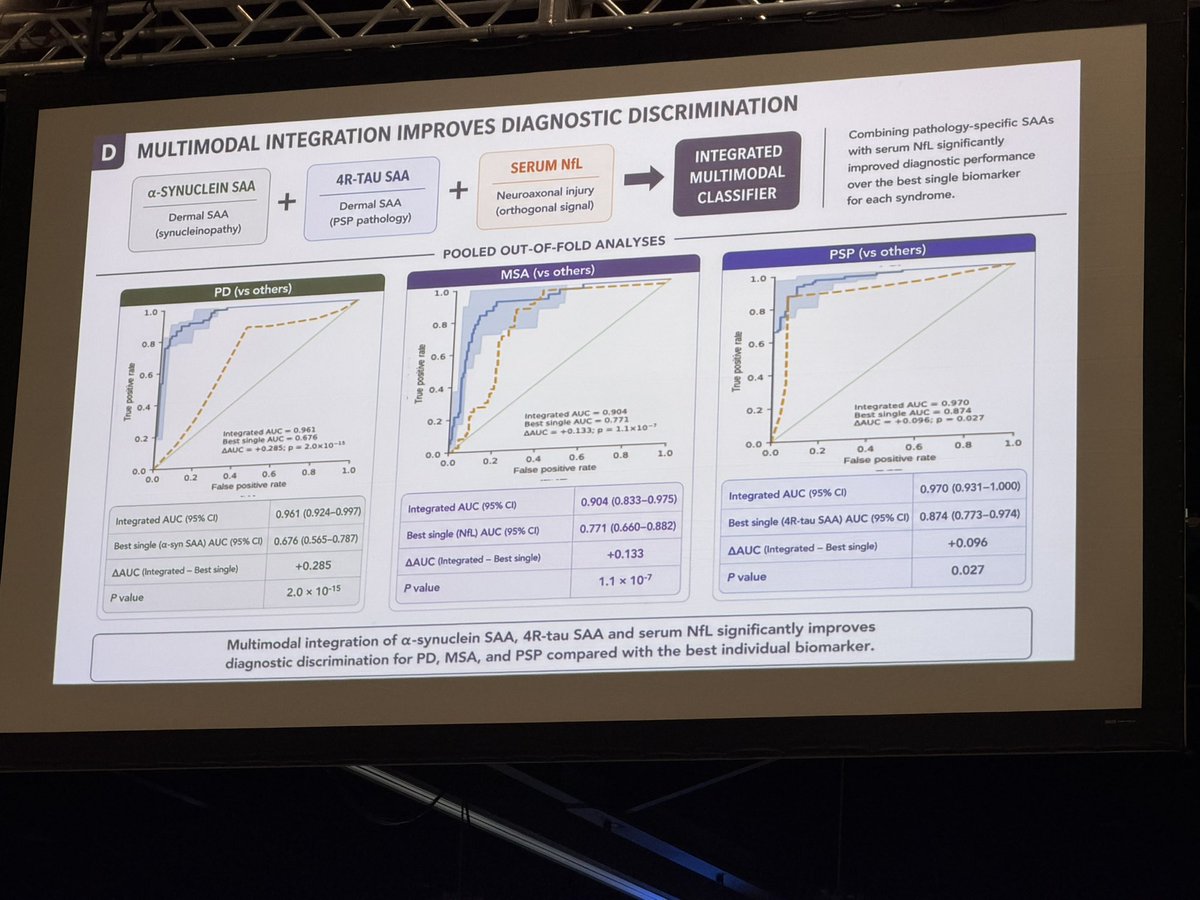
Big challenge in Parkinson’s is that synuclein seeding assays can be positive across many diseases. Nice plenary this morning showing how this group uses synuclein seeding + 4 R TAU + NFL to sort this out using a multi-modal biomarkers approach. This is one such approach used at the University of Toronto and presented today at the World Parkinson Congress.
Cervical dystonia has 2 big phenotypes:
-Early onset (35y) = much worse pain/mood/QoL vs later onset (48y) — motor severity differences are smaller.
-Don’t “BoNT-and-bye”: treat the non-motor load. https://t.co/TbYDNbv70S
Cullinane et al. identify three subtypes of progressive supranuclear palsy with different progression patterns and show that sex, genetic variation, and co-pathology influence tau distribution and clinical phenotype. https://t.co/guvesxVzx7
World Parkinson’s Day may have taken place over the weekend (April 11th), but raising awareness doesn’t stop there 💙
This important day is a reminder of the strength, resilience, and community behind those living with neurological conditions🧠
#WorldParkinsonsDay
We are very proud of this achievement! Congratulations to @LucaMarsili1, @AMahajanMD, @AlbertoEspay, and the other faculty and co-authors of this award-winning manuscript! 🎉🧠
Did you know AD pathology also impacts PD and related disorders? This review underscores the impact of aβ and tau co-pathology on clinical progression and heterogeneity in PD and atypical parkinsonism, emphasizing the value of biomarker approaches.
https://t.co/s82jE8Vfcs
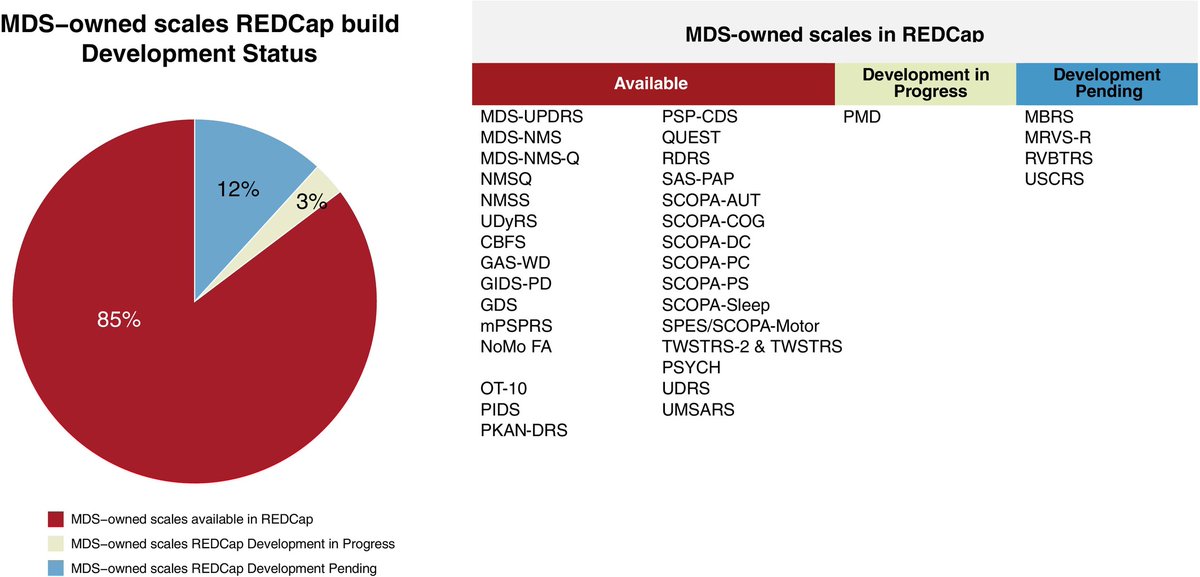
Several MDS rating scales now have official versions within REDCap, thanks to efforts by the Electronic COA Committee to promote compliance and uniformity in clinical research. @MDJ_Journal https://t.co/UQUBHwyVoj
Our group just published the First Saudi data on fatigue in Parkinson’s disease:
• 61% had significant fatigue (FSS ≥4)
• Fatigue linked to non-motor symptoms
• Higher risk with low physical activity and low water intake
https://t.co/raI6i5QubY #ParkinsonsDisease#Fatigue
Recurrent “delirium”, normal scans, fluctuating cognition - sound familiar?
Our recent review shows why dementia with Lewy bodies is often hiding in plain sight, and how to recognise it early in clinic and on the ward.
🔓 Open access: https://t.co/VYKaUqdERI
#Neurology #OpenAccess #FOAMed
🧠𝗗𝗼 𝘆𝗼𝘂 𝗹𝗶𝘃𝗲 𝘄𝗶𝘁𝗵 𝗣𝗮𝗿𝗸𝗶𝗻𝘀𝗼𝗻’𝘀 𝗱𝗶𝘀𝗲𝗮𝘀𝗲?
We want to hear your views on technology! 💬
💡 Your experience can shape future tools and research
👉 https://t.co/vLmn8i1QXP
#ParkinsonsDisease#PDresearch#ParkinsonsAwareness
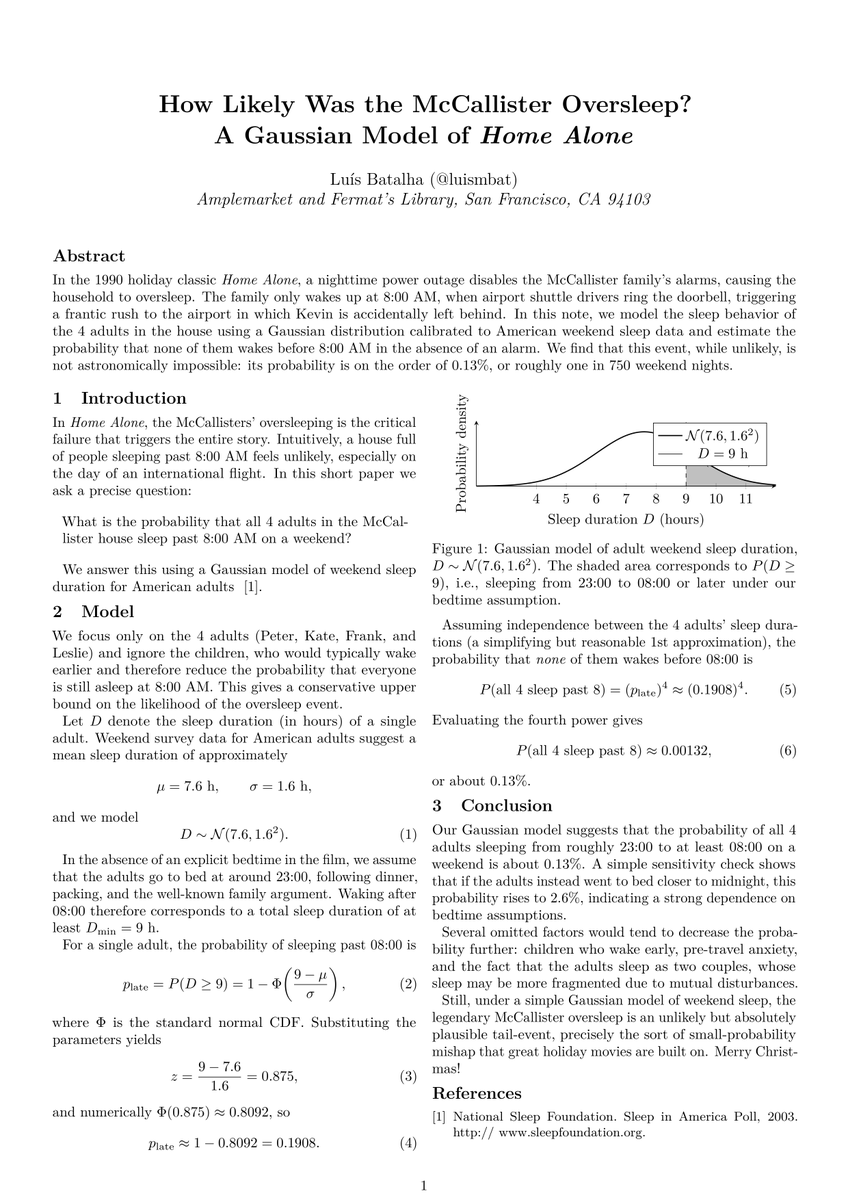
After rewatching Home Alone, I couldn’t stop wondering:
how plausible is the oversleep that leaves Kevin behind?
So I wrote a tiny paper and ran the numbers.
Merry Christmas! 🎄
Foslevodopa infusion in the real world has shown promise for Parkinson's, however we must pay attention to any emergent neuropsychiatric symptoms. Continuous subcutaneous infusion refers to medication delivered under the skin at a steady rate to smooth out motor fluctuations. This research letter provides important insights into safety signals that may emerge when folks start and adjust this therapy at home. Maeve Bradley and colleagues describe in Movement Disorders Clinical Practice their extended real world experience w/ foslevodopa foscarbidopa using an outpatient titration protocol.
Key Points:
- Outpatient initiation was feasible, however dose optimization still required several weeks and infusion rates increased by an average of 35% from baseline.
-Neuropsychiatric complications were more frequent w/ hallucinations emerging in 21 percent of patients and frequently appearing weeks after initiation.
- Discontinuation rates were similar to inpatient programs, however reasons differed and included neuropsychiatric symptoms, infusion site issues and lack of effectiveness.
My take: We will need to provide guidance on when to employ pump therapies in Parkinson's and what to do if neuropsychiatric symptoms emerge. Real-world data is really important to this effort. Here are 5 points that resonated w/ me: 1- Expect individualized dosing because stable infusion rates usually take weeks to achieve and will require close follow up. 2- Watch for delayed hallucinations because these symptoms may appear long after the first few days of treatment and require rapid adjustment. 3- Understand the role of past psychosis since a history of hallucinations may increase risk, however does not perfectly predict who will struggle. 4- Rely on your care team because trained nurses visiting at home can safely guide adjustments and keep therapy on track. 5- Recognize when to stop because some folks will discontinue due to neuropsychiatric issues or skin reactions, and switching therapies may be the best option for some folks.
https://t.co/poGV5mHjYO @ParkinsonDotOrg@FixelInstitute@PdAvengers@ACPIMPhysicians@movedisorder
It was wonderful having you in Dublin. A masterclass in itself! Your grand rounds performance was a tour de force. We’ll have to find even more complex cases next year!
Thank you, @FearonConor for your friendship and for leading with Tim Lynch and Dublin team a splendid Irish PD & Movement Disorders Master Class. I learned from the many cases presented and the Grand Rounds. Eternally grateful. 🙏🏻❤️