Marriott is quietly hoping you never learn how their loyalty program actually works.
I did.
There's $1,800/year in free upgrades, free nights, and hidden rate codes sitting inside the same Bonvoy account most guests use for nothing except checking in.
One woman sent a single email before her stay. Marriott upgraded her to a $3,000 suite. For free.
Most guests book on Expedia, check in, check out, and never touch the 9 features Marriott buries behind the login screen.
Here's the full playbook 🧵
Remember this post and the points I made below regarding Insight trial and the authors that critiqued DCVax-L results? Well Marnix Bosch PhD from NWBO made the same point in this slide today, saying that those authors who criticized the JAMA article for using cohort level data because individual patient data was not available when on to show that PSM was the best standard, which Bosch agrees with and goes on to show how DCVax-L data kicks more ass with PSM data. Love me that nectar of poetic justice.
Rahman and Trippa who criticized the DCVax-L external control arm in 2023 will now to have eat their own words.
The trial they reanalyzed is the INSIGhT trial (Individualized Screening Trial of Innovative Glioblastoma Therapy).
The findings were published in the Journal of Clinical Oncology in May 2026, with Dr. Lorenzo Trippa and Dr. Rifaquat Rahman (from Mass General Brigham / Dana-Farber) as co-senior authors.
This specific paper is the smoking gun that mathematically validates the entire regulatory strategy Northwest Biotherapeutics is currently executing. Here is exactly what they did, how it worked, and why it matters.
The INSIGhT Trial Reanalysis
The original INSIGhT trial was a randomized Phase II platform trial for newly diagnosed, MGMT-unmethylated glioblastoma. The trial tested three different experimental drugs against a standard-of-care internal control arm.
The original results for all three drugs were a failure. Compared to the internal randomized control group, none of the three drugs—abemaciclib, neratinib, or CC-115—improved survival.
What the Harvard Team Did:Trippa, Rahman, and their team wanted to see if they could recreate a randomized trial without actually using the randomized controls.
They took the survival data for the patients who received the three experimental drugs.
They threw out the trial's internal randomized control arm.
They replaced the internal controls with Individual Patient Data (IPD) sourced from outside real-world datasets and historical clinical trials.
They ran a strict Propensity Score Match (PSM)—the exact same statistical method Marnix Bosch is presenting at BNOS—to perfectly match the external control patients to the experimental patients.
The Results: The Propensity Score Match worked flawlessly. When compared against the matched external controls, the hazard ratios came back at 1.00 for abemaciclib, 0.93 for neratinib, and 0.88 for CC-115.
The external control data reproduced the exact same "null" result as the gold-standard randomized control arm. It proved that the drugs didn't work, matching reality perfectly.
Why This is the Ultimate Defense for NWBO
When you look at the INSIGhT reanalysis in the context of the DCVax-L timeline, it creates a massive, inescapable paradox for the critics of Northwest Biotherapeutics.
1. It Proves External Controls Are Valid in Glioblastoma. Historically, skeptics argued that glioblastoma is too complex to use external controls because survival relies heavily on variables like the extent of surgical resection. The INSIGhT paper proved that as long as you have the raw patient-level data and run a strict Propensity Score Match, external controls are just as accurate as an internal placebo arm.
2. The Critics Authored the Validation In 2023, Trippa and Rahman were the loudest critics of the DCVax-L Phase 3 data, writing a peer-reviewed letter in JAMA Oncology arguing that NWBO's external control method (MAIC) was statistically weak.
In May 2026, those same two statisticians published the INSIGhT paper proving that Propensity Score Matching with patient-level data is the undeniable gold standard for glioblastoma trials.
3. The Checkmate: When Marnix Bosch takes the main stage at BNOS in July 2026 to present the DCVax-L data, the title of his talk literally promises a Propensity Score Match analysis.
NWBO has adopted the exact statistical framework that their harshest critics just validated. If the BNOS presentation shows that DCVax-L's survival curves hold up under PSM, Trippa and Rahman cannot attack the math without attacking their own INSIGhT publication. It traps the skeptics in their own methodology and hands the MHRA peer-reviewed proof that the DCVax-L statistics are legally and scientifically sound.
$NWBO Per co-pilot when trying to assess regulatory strength/risk beyond MHRA and potential of increased M&A activity.
Yes, it could increase the probability of partnering or acquisition interest from large pharma, but I would characterize it as a reduction in risk rather than a transformation of DCVax-L into a risk-free asset.
Why Big Pharma Might View This Favorably
Historically, the biggest concerns around DCVax-L have been:
External control arm methodology
Lack of a traditional randomized contemporaneous control
Questions about causality versus association
Regulatory uncertainty in major markets
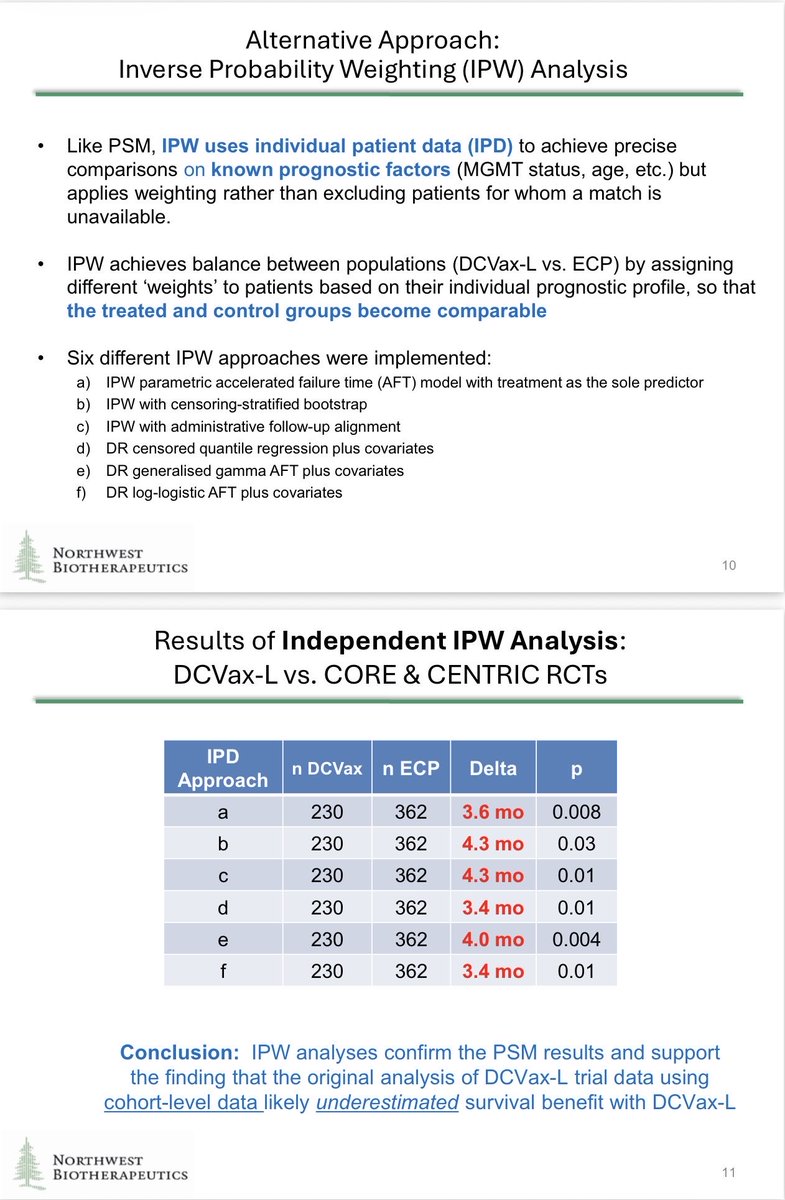
The BNOS presentation directly addresses the first three issues through patient-level propensity score matching (PSM), inverse probability weighting (IPW), and sensitivity analyses. The analyses consistently found a survival benefit across multiple independent datasets and suggested the original published benefit may have been underestimated. [NWBT-BNOS-...-FINAL-v02 | PDF]
For potential acquirers, that's important because they generally discount assets not only for clinical risk, but also for statistical controversy risk and regulatory risk.
Impact on FDA, EMA and Other Regulators
The new analyses do not eliminate regulatory risk.
However, they potentially strengthen arguments that:
The survival effect is real.
The effect is reproducible across multiple external datasets.
Results are not driven by obvious confounding.
The original statistical analysis plan contemplated such IPD analyses if data became available. [NWBT-BNOS-...-FINAL-v02 | PDF]
That matters because FDA, EMA, MHRA, Health Canada and other agencies often focus heavily on whether observed treatment effects could be explained by bias.
If regulators ultimately accept these patient-level analyses as valid supporting evidence, the probability of rejection based solely on external-control concerns may be lower than many bears previously assumed. However, regulators still must evaluate manufacturing, CMC, potency assays, consistency of production, safety, and overall benefit-risk. The BNOS data primarily strengthen the efficacy package. [NWBT-BNOS-...-FINAL-v02 | PDF]
Why This Could Attract Pharma Interest
For a large oncology company, DCVax-L potentially offers:
A platform relevant beyond glioblastoma.
Personalized cellular immunotherapy know-how.
Combination opportunities with checkpoint inhibitors.
Potential expansion into additional solid tumors.
Orphan oncology economics.
The presentation itself specifically highlights future combination opportunities with checkpoint inhibitors and immune stimulants. [NWBT-BNOS-...-FINAL-v02 | PDF]
Large pharma often becomes interested when three elements start aligning:
FactorBefore IPD analysesAfter IPD analysesClinical signalPositive but debatedPositive and potentially more robustStatistical controversyHighReducedRegulatory visibilityUncertainPotentially improvedAcquisition attractivenessModerateHigher
What Could Trigger Actual Offers
The events most likely to trigger serious discussions would be:
Positive MHRA outcome
Validation from independent regulators
Formal incorporation of the new IPD analyses into regulatory review
Evidence that manufacturing review is progressing successfully
Additional combination-trial data
If MHRA were to approve DCVax-L first, many pharma companies would likely view that as external validation of both the clinical data and manufacturing platform. That could have a much larger impact on partnering interest than the BNOS analyses alone.
My Bottom-Line Assessment
Before these new analyses, a skeptical acquirer could argue:
"The apparent survival benefit may be largely due to external-control bias."
The BNOS presentation makes that argument substantially harder to maintain because multiple patient-level matching approaches, IPW analyses, and sensitivity analyses point in the same direction. [NWBT-BNOS-...-FINAL-v02 | PDF]
As a result, I would view the new data as:
Increasing the attractiveness of DCVax-L as a partnering/acquisition target
Reducing perceived regulatory risk across MHRA, FDA, EMA and other agencies
Improving confidence that the efficacy signal is genuine
But I would not yet say it makes a buyout inevitable. In biotech M&A, the single biggest value inflection would still likely be first major-market approval, especially MHRA approval if it occurs, because that would convert a regulatory hypothesis into a regulatory fact.
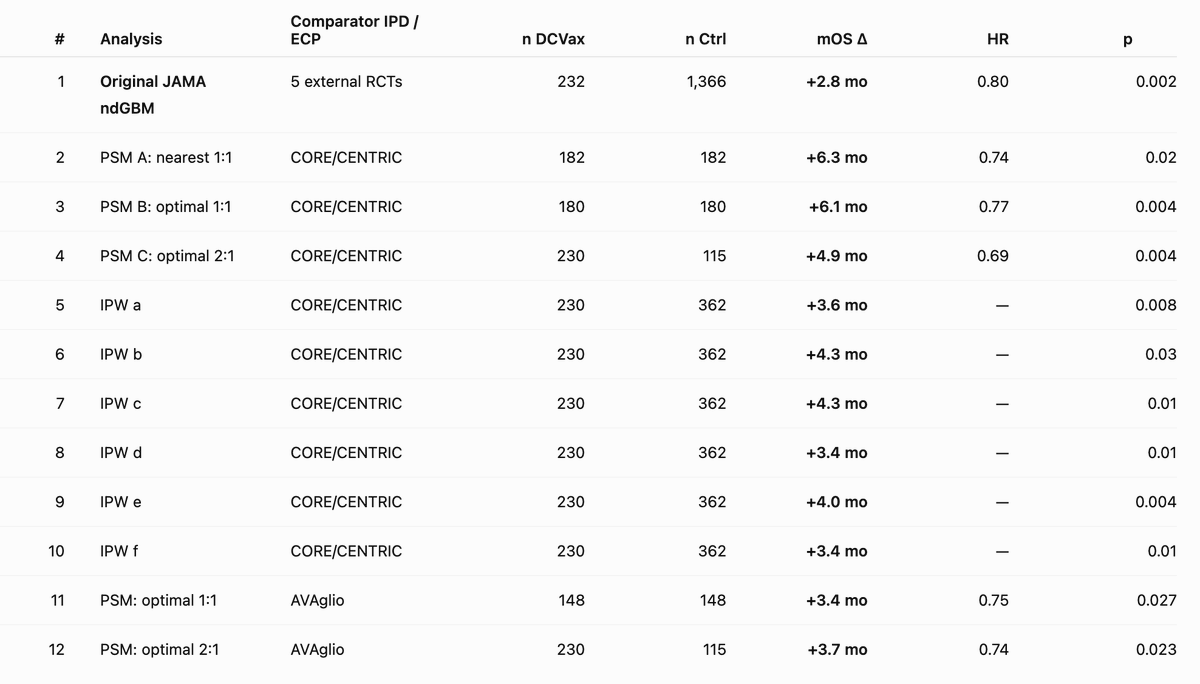
PSM analysis using Individual Patient Data shows a OS benefit associated with DCVax-L treatment to be meaningfully longer (between 3.4 and 6.3 months) than the 2.8 months in the original analysis
Further enhancements to OS is seen in combining DCVax-L with Hiltonol® #DCvax $NWBO
New IPD-based PSM/IPW methods estimate a +3.4 to +6.3-month mOS benefit for DCVax-L in ndGBM across 11 survival analyses. For context, the original JAMA cohort-level analysis showed a +2.8-month mOS benefit — suggesting the original estimate may have been conservative. Importantly, these analyses were anticipated in the SAP.
$NWBO Northwest Biotherapeutics. DCVax-L, an autologous dendritic cell cancer vaccine awaits MHRA decision for glioblastoma. Wave of combination studies anticipated.
https://t.co/MjrUICgKGo
😱 MASSIVE UPDATE BNOS PRESENTATION SUMMARY!😱
DCVax-L is starting to look like one of the most misunderstood stories in biotech.
The latest BNOS analysis doesn’t just confirm efficacy — it suggests the Phase 3 trial significantly UNDERSTATED it. #NWBO#DCVAX 💎💎💎
🟥American Resilience and Optimism Despite Inevitable Attacks On U.S. Soil
"I really don't think the terrorists have any understanding of what they're going to be up against here. They think it's going to be easy and I don't feel that's the case." - Sarah Adams
"Now, I know attacks are going to happen here. I'm very clear-eyed about I know people are going to die. I'm focused on let's minimize the deaths. Like I'm at that stage now. The optimism is gone that we're going to thwart it. But, I do feel we have, you know, made an America where people will do something" - Sarah Adams
"Well, I mean, I think like we all saw 9/11, right? Like I know there's all these Americans who are going to step up and be heroes and we built this whole warrior class for 20 years. So, I'm actually very optimistic. - just recently we had the strange guy in the plane try to open the cockpit and then the air marshal fighter pinned him in the seat. Like that's the America we are today. And so, I am a little excited about that piece because, hey, come here. Like we'll put you down. Like I really don't think the terrorists have any understanding of what they're going to be up against here. They think it's going to be easy and I don't feel that's the case." - Sarah Adams
Sarah Adams (Former CIA): Here's What's Actually Happening With Iran Right Now
@sarahadams X @ThisIsIRONCLAD
https://t.co/sZBw3PZ91L
🟥Birthright Citizenship: A Channel For Hostile Actors To Manufacture U.S. Citizens
"The existence of even a small but real channel for hostile actors to manufacture U.S. citizens is an unacceptable risk. Hostile adversaries do not need the majority of births to be part of a grand conspiracy. They only need the ability to use the system when it serves their interests."
"The hard truth is that governments must choose what they favor when values conflict. You either favor the innocent children of economic migrants accepting the security risks that come with it OR our nations long-term security by closing or narrowing this loophole, even if it means innocent cases are affected."
"Seven years from now, more or less, the Social Security system will go bust. There isn’t enough coming in from people still working to cover the benefits going to people who are retired," per Forbes.
STROKE at the age of 34.
Runs 5k on weekends.
Normal blood pressure.
No diabetes. No smoking.
But ONE common stress relief habit quietly tore a major blood vessel and caused a massive brain attack.
A medical thread on what actually happened 👇
$NWBO High-Grade Glioma Market Witnesses Strong Momentum During the Forecast Period (2026-2036) with Increasing Clinical Activity and Drug Development | DelveInsight
https://t.co/F5LKeq0LJz
From Fruita, CO near Grand Junction. This fire was started by lightning last night in Utah. 10% humidity and westerly winds up to 46 mph has driven the fire towards us. Gonna be a long summer.