Gene editing is finally here.
And it's targeting the biggest killer in the world. Heart disease.
Eli Lilly $LLY just released data for a gene therapy called VERVE-102.
It completely changes how we treat high cholesterol.
Instead of taking a pill every day, you get one single IV infusion. The medicine travels directly to your liver. It permanently turns off the specific gene that causes high LDL cholesterol.
The early trial results are incredible. Patients experienced a massive 60% drop in their LDL cholesterol.
Think about what GLP-1 drugs did for obesity.
Five years ago, Ozempic was "just Phase 2 data." People said the side effects were unclear. The long-term outcomes were unknown.
Now it's a $50 billion/year drug that changed how we treat obesity.
GLP-1s rewrote obesity. VERVE-102 could rewrite heart disease.
Medicine is moving faster than most people realize.
One injection, 62% lower LDL - permanently. Gene editing for cholesterol is here.
.@cremieuxrecueil is correct. Besides GLP-1 antagonist like Ozempic or, more recently, Retatrutide, this is probably the next breakthrough that is almost impossible to put into words.
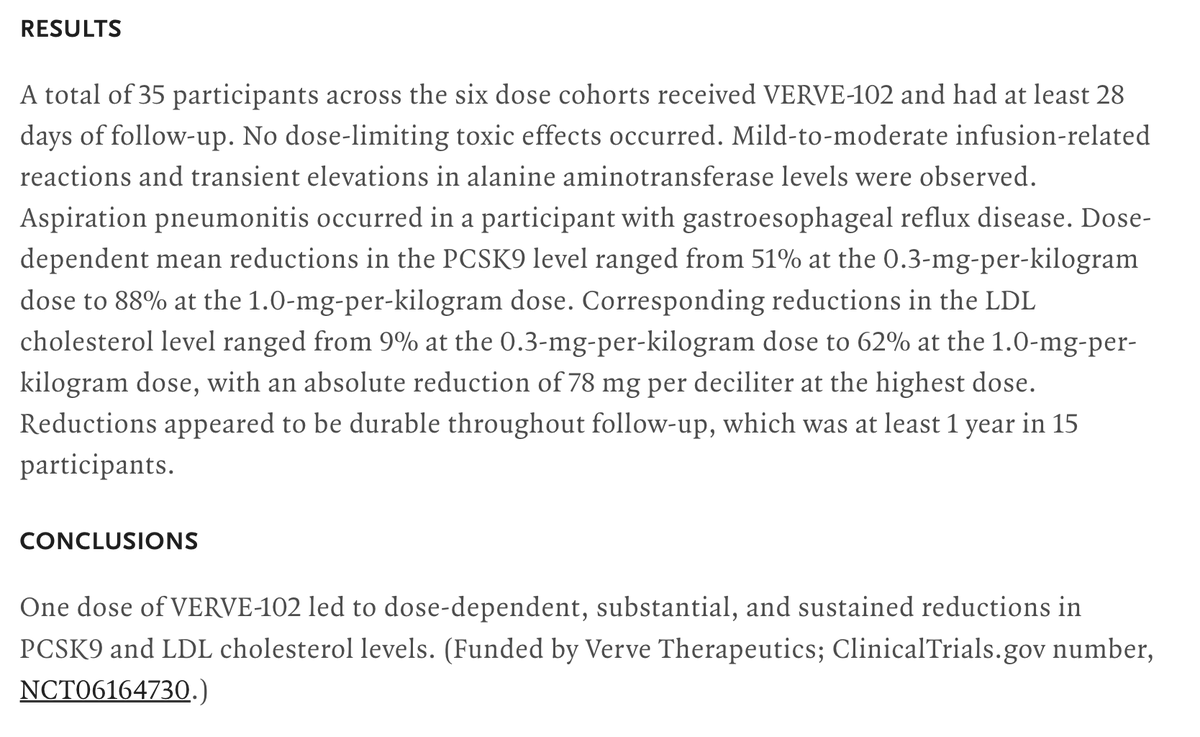
Verve Therapeutics (Eli Lilly) just published Phase 1 results for VERVE-102 in the NEJM.
It's a single-infusion base-editing therapy that inactivates PCSK9 in the liver. At the highest dose, PCSK9 dropped 88% and LDL cholesterol fell 62%. Reductions held for at least a year.
35 patients with familial hypercholesterolemia or premature coronary artery disease. No dose-limiting toxicities. Main side effects: mild infusion reactions and transient liver enzyme elevations.
Still Phase 1, still small, no cardiovascular outcome data yet. But the proof of concept for permanent, one-shot LDL reduction via gene editing is real.
This is an absolute game changer and im not exaggerting.
Elevated LDL cholesterol is responsible for an estimated 4.4 million deaths every year worldwide and remains the single biggest modifiable driver of cardiovascular disease, the leading cause of death globally.
Why MID-35 from Kimera Chems is FAR superior to FLGR242 from BioLongevity Labs for myostatin research!
Think of myostatin like the body’s built-in “brakes” on muscle growth — it tells your muscles “that’s enough, stop getting bigger.” Both compounds try to release those brakes, but they do it in totally different ways.
MID-35 (the D-peptide from Kimera) is like a super precise key that snaps right onto myostatin and neutralizes it directly. It’s super stable (thanks to its D-peptide design), sticks around longer, and focuses almost entirely on myostatin without messing with other similar signals in the body. In preclinical stuff, this leads to cleaner, more targeted muscle growth effects.
FLGR242 is a tweaked version of follistatin (a natural myostatin blocker). It works by grabbing myostatin (and potentially other stuff) to stop it from working. The tweak helps it avoid binding to activin, which is cool for reducing some side effects, but it’s still a broader approach compared to MID-35’s laser focus.
Bottom line: MID-35 feels like the more efficient, modern tool for straight-up myostatin blocking with great stability and potency at a fraction of the price for similar research amounts.
Real value for researchers chasing serious gains.
Save up to 20% with code ELEVATE — plus stack it with their 30% off sitewide sale from 5/22-5/26!
Link in bio / https://t.co/nY9GP4OYAx
#Biohacking #Myostatin #MuscleResearch #KimeraChems #ElevateBiohack
MID-35: The Myostatin Peptide Nobody’s Talking About
Myostatin inhibition is everywhere right now.
Every page is pushing follistatin… and yeah, it’s a real pathway.
But there’s another compound in this space that deserves way more attention:
MID-35
⸻
What is MID-35?
MID-35 is a 16-amino acid retro-inverso D-peptide developed at the Tokyo University of Pharmacy and Life Sciences and published in ACS Medicinal Chemistry Letters.
This isn’t influencer hype. It’s peer-reviewed medicinal chemistry.
The key difference?
It uses D-amino acids — mirror-image structures that enzymes don’t easily break down.
Result:
→ Significantly improved stability
→ Longer functional lifespan vs traditional peptides
→ More resistant to degradation than L-peptides like MIPE-1686
MW ~2,350 Da — small, efficient, purpose-built.
⸻
How it works
MID-35 directly targets myostatin at the receptor level.
Instead of broadly interfering with pathways, it:
→ Binds the activin receptor site
→ Blocks downstream Smad 2/3 signaling
→ Releases inhibition on PI3K/Akt/mTOR (muscle protein synthesis)
→ Reduces Atrogin-1 + MuRF1 (muscle breakdown signals)
In simple terms:
You’re removing the brake AND easing off the destruction signal
⸻
What the data shows
Preclinical research models show:
→ ~1.3x increase in muscle weight (28 days, single injection)
→ ~1.25x increase via transdermal delivery (iontophoresis)
→ Improved strength, food intake, and survival in cachexia models (when combined with ghrelin pathway agents)
Multiple studies. Multiple models. Reproducible outcomes.
⸻
MID-35 vs Follistatin (FLGR242)
MID-35
→ Direct myostatin binding
→ More targeted mechanism
→ Higher selectivity in studies
→ Built-in protease resistance (D-peptide design)
→ Backed by published research
FLGR242 (Follistatin-based)
→ Broad ligand binding (TGF-β family)
→ Less selective by nature
→ Complex recombinant structure
→ Limited independent published data (mostly marketing-driven)
Different tools. Different approaches.
But one is clearly more mechanistically precise.
⸻
Why this matters
We’re in a phase where GLP-driven weight loss is exploding…
…but muscle preservation is lagging behind.
MID-35 represents:
→ Targeted myostatin modulation
→ Cleaner signaling approach
→ Strong stability profile
→ Real published data (not just marketing)
This is what actual medicinal chemistry looks like when done right.
⸻
Available soon
2–3 weeks
https://t.co/nY9GP4OYAx
⸻
Research Use Only
Not for human consumption. Intended strictly for laboratory and analytical research.
New to the Kimera catalog: MID-35.
https://t.co/5l9xXRH24m
Myostatin Inhibitory D-Peptide-35. The first and only retro-inverso D-peptide myostatin inhibitor with published in vivo data on increased skeletal muscle mass.
What it is:
A 16-amino-acid synthetic D-peptide engineered to block myostatin (GDF-8), the dominant negative regulator of skeletal muscle growth. Developed at Tokyo University of Pharmacy and Life Sciences through iterative SAR work, characterized across three peer-reviewed papers (ACS Med Chem Lett 2022, Cancer Science 2022, Pharmaceuticals 2023).
Why it's different:
Every other myostatin tool peptide on the market is an L-peptide. They get chewed up by proteases in minutes. MID-35 is built retro-inverso, sequence reversed and every residue in the D-configuration. The spatial geometry that lets it bind myostatin is preserved. The proteolytic susceptibility is not.
The mechanism is clean too. It binds myostatin at the activin type I receptor interface, blocking Smad2/3 signaling without broadly neutralizing other TGF-beta superfamily ligands like activin A, GDF-11, or BMP9/10. That selectivity is what separates it from decoy receptor approaches and broad-spectrum inhibitors like follistatin.
The numbers:
- IC50 of 0.19 uM in Smad-responsive luciferase reporter assays
- Approximately 20x more potent than its predecessor (peptide-2, IC50 4.1 uM)
- 1.25-fold increase in tibialis anterior muscle mass after 28 days in C57BL/6J mice
- Combination with anamorelin improved grip strength and survival in cancer cachexia models
This is a tool peptide for muscle biology, sarcopenia, and TGF-beta pathway research. Not a clinical asset. Not an L-peptide novelty. Genuinely new chemistry with published preclinical data behind it.
HPLC verified. Lyophilized. Third-party tested.
$299.99 per vial.
Research use only. Not for human consumption.
Code KIMERA10 for 10% off
MID-35 Analysis: Overcoming Myostatin Constraints
Standard L-peptide configurations often suffer from rapid enzymatic cleavage, limiting their utility in extended biological tracking.
MID-35 addresses this vulnerability directly through its unique retro-inverso construction. By combining D-amino acids with an inverted sequence topology, it maintains the precise spatial orientation required to bind and neutralize myostatin (GDF8) while remaining virtually invisible to proteolytic enzymes.
For laboratories running long-term cellular development protocols, MID-35 represents a massive leap forward in experimental stability. Review the analytical data and secure your batch during the weekend event by following the link below.
Use code ELEVATE to save 20% now! 10% more with BTC.
#MID35 #PeptideResearch #ResearchPeptides #ResearchChemicals #RUO #ResearchUseOnly #Biohacking #LongevityResearch #Nootropics #CognitiveResearch #NeuroResearch #MolecularResearch #BiotechResearch #ExperimentalCompounds #PerformanceResearch #ScientificResearch #LabResearch #AdvancedResearch #MechanismOfAction #ResearchCommunity #ResearchDriven
🚨 Anthropic just showed a 27-minute workshop on how to actually do prompts for Claude.
Taught by the people who built it.
Free. No registration. No paywall.
I've seen $300 courses that don't cover what they teach in the first 8 minutes.
Watch it and bookmark it now.
Eli Lilly released retatrutide Phase 3 data yesterday. 28% weight loss in 80 weeks. The most powerful obesity drug that’s ever been tested.
And today the cancer signal drops.
12,112 patients. Seven tumor types. GLP-1 users had half the lung cancer metastasis rate (10% vs 22%). Breast cancer: 43% cut. Colon cancer five-year mortality in a separate study: 15.5% vs 37.1%.
Cancer joins a list that already includes heart disease (SELECT, 20% MACE reduction), kidney failure (FLOW, 24% slower decline), sleep apnea (SURMOUNT-OSA, FDA-approved), addiction (BMJ, 600K veterans, 18-25% reduction across substances), and liver disease (86% fat clearance).
Tumors express GLP-1 receptors. Activate them and NF-kB drops, apoptosis rises. The drug isn’t just shrinking fat. It’s talking directly to the cancer.
One drug class. Designed for blood sugar. The biology keeps finding uses the designers didn’t predict.
Première mondiale ! Un robot a travaillé 200h non-stop, et trié plus de 249 000 colis à lui seul. Pas une seule panne, pas une seule pause et tout a été diffusé en live pour le prouver.
À la base c'était un défi de 8h. Le robot a tellement bien tourné qu'ils ne l'ont jamais coupé. 200 heures plus tard il tournait encore.
Le truc de fou, c'est qu'il y a quelques jours un stagiaire a fait un duel contre le robot sur un shift de 10h. Le gars a gagné. De justesse, 2.79 secondes par colis contre 2.83 pour la machine. Sauf que le stagiaire a fini avec l'avant-bras en vrac. Le robot lui il a continué 190 heures de plus sans broncher.
Et c'est là que je comprends pas. On a littéralement un robot humanoïde qui fait un boulot d'entrepôt en continu, sans supervision, tout est géré par son IA embarquée. Si le robot bug, il se reset tout seul et reprend. Si il a un souci hardware, il sort de la ligne et un autre prend le relais automatiquement.
Malgré tout ça, la majorité des gens ne voient pas ce qui arrive. On scrolle, on passe, on se dit "c'est cool" et on oublie. Mais c'est pas "cool". C'est un changement de civilisation. Les tâches physiques répétitives vont être automatisées.
La robotique humanoïde c'est le sujet dont personne ne parle assez. On commence à peine à parler d'IA avec bien du retard, sauf qu'il faut comprendre que l'étape d'après c'est l'IA incarnée, cad, les robots.
@shubh19 Behind every AI restructuring headline are thousands of ppl wondering wht to do nxt
Fr companies, it’s cost cutting.
Fr employees, it’s someone’s entire life changing overnight
The scariest part about AI isn’t the technology
It’s hw fast it’s replacing ppl before they can adapt