Knowledge of anatomy is vital to evaluate the PNS!
ESHNR Webinar on “Perineural spread in head and neck malignancy“ today!
🎤 Speaker: Anbarasu Arangasamy, Coimbatore/IN
👨🏫 Moderator: @jussihirvonen, Turku/FI
If you are only looking at the optic nerve on Orbital MRIs, you need to open your EYES!
Don’t be blind to all the other nerves in the orbit!
Branches of trigeminal V1 &V2 and the oculomotor nerve all can cause pathology in the orbit
But if you don’t look, you won’t see!
Let this figure show you some of the nerves you can see in the orbits (CN6 is only seen proximally bc its orbital course is so short & CN4 is too small to reliably see)
Hopefully, now you will have an eagle eye when it comes to orbital pathology!
A premature label of Bell’s palsy is a frequent source of medical error, delaying diagnosis of a more nefarious cause of facial palsy. Lack of recovery in 2-3 months, or a history of head and neck or cutaneous malignancy, should prompt more workup.
@LizzRad at #ASHNR25
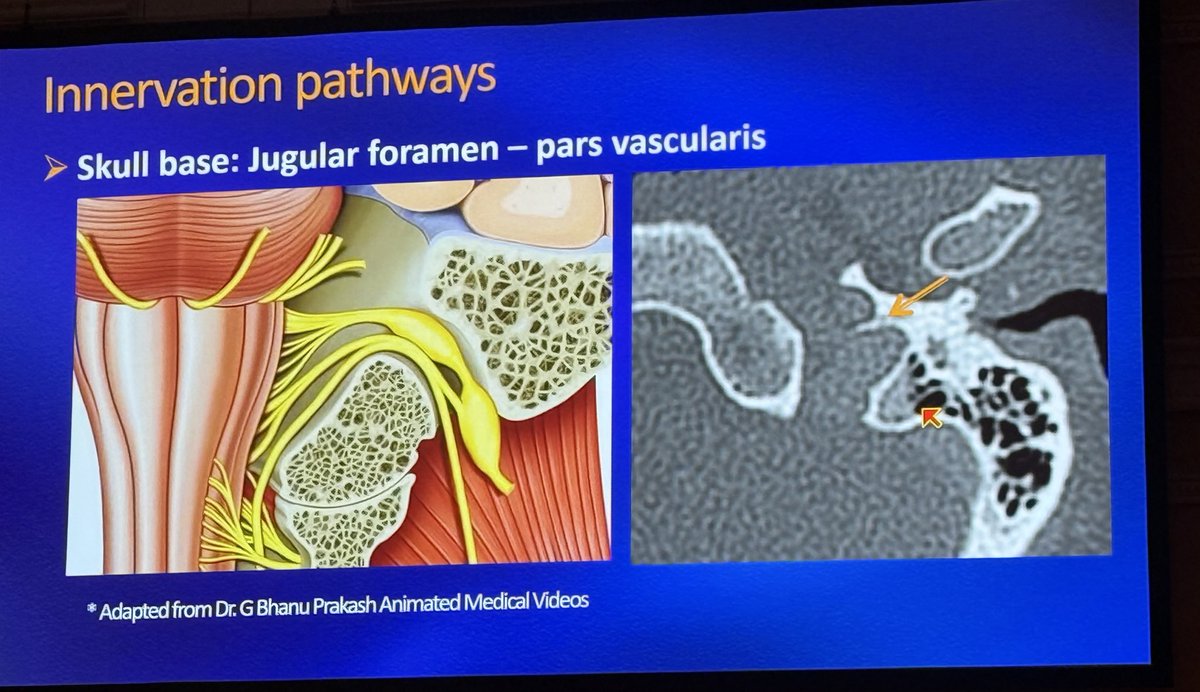
Interesting pearl from @IlonaSchmalfuss excellent lecture on vocal paralysis at #ASHNR25 :
Preservation of the jugular spine (arrow) helps distinguish a normal asymmetric enlarged jugular foramen from jugular foramen lesions that cause remodeling or destruction.
@ASHNRSociety
DOTATATE PET is exquisitively sensitive for small volume neuroendocrine neoplasms and is useful for the staging or surveillance of olfactory neuroblastoma, paraganglioma, etc.
@DShatzkes at #ASHNR25
Great breakdown of perineural tumor spread from @StillGinz at #ASHNR25
A few key points:
-A Bell’s palsy only becomes Bell’s palsy when it goes away.
-Widened mental foramen suggests perineural dz rather than direct bone invasion.
#ashnr#asnr#neurorad@ASHNRSociety