There's a tiny ion channel in your body that's involved in migraines, chronic fatigue, long Covid, and pain sensitivity — and most people have never heard of it.
Meet TRPM3. 🧬
TRPM3 is a calcium ion channel that sits on your nerve cells and acts like a heat alarm. When it detects high heat — or certain neurohormones — it opens up and lets calcium flood in, which signals pain in sensory neurons.
But TRPM3 doesn't just handle heat. It's also involved in:
- Migraine signaling
- Insulin release from the pancreas
- Blood vessel constriction
- Immune cell function
- Glutamate balance in the brain
One channel. A lot of effects.
The migraine connection is fascinating — especially for women.
Progesterone suppresses TRPM3. When it drops during your cycle, TRPM3 becomes more active and triggers CGRP release in the trigeminal nerve.
CGRP is a key driver of migraines. This is the biological chain.
Here's where it gets really interesting: #MECFS
Studies show that ME/CFS patients have reduced TRPM3 function on natural killer (NK) cells.
NK cells need calcium influx through TRPM3 to release the granules that kill virus-infected cells. Less TRPM3 = blunted immune response. TRPM3 also affects blood pressure response and glutamate/GABA homeostasis.
The same TRPM3 dysfunction is now showing up in #longCovid patients too.
Fatigue, brain fog, post-exertional malaise, pain — symptoms that overlap heavily with ME/CFS.
Here's the hopeful part: a 2025 study showed that low-dose naltrexone (LDN) can restore TRPM3 function in long Covid and ME/CFS patient cells — within 24 hours.
LDN blocks the mu-opioid receptor, which normally suppresses TRPM3. Remove the block, restore the function.
Your genetics also matter here. Multiple variants in the TRPM3 gene are associated with increased ME/CFS risk. Others affect migraine susceptibility and pain sensitivity.
Check out the full article for all the details, look at your TRPM3 variants, and see the solutions (natural and medications) that interact with TRPM3.
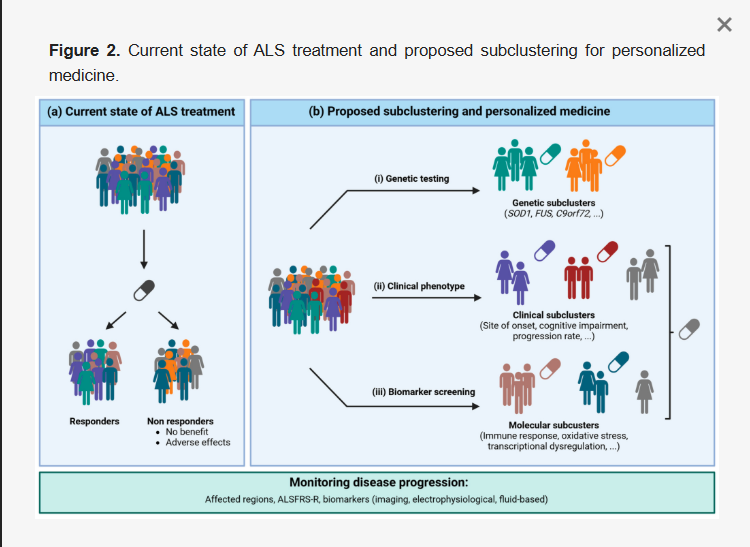
This paper is an amazing read. I think it's free to read, and also clearly classifies the ALS pathology and calls out why we need to have precision medicine for ALS.
We need to shift our thoughts from one universal cure to many cures.
Reevaluation of past clinical trials and drugs with specific subgroups based on ALS type should be performed.
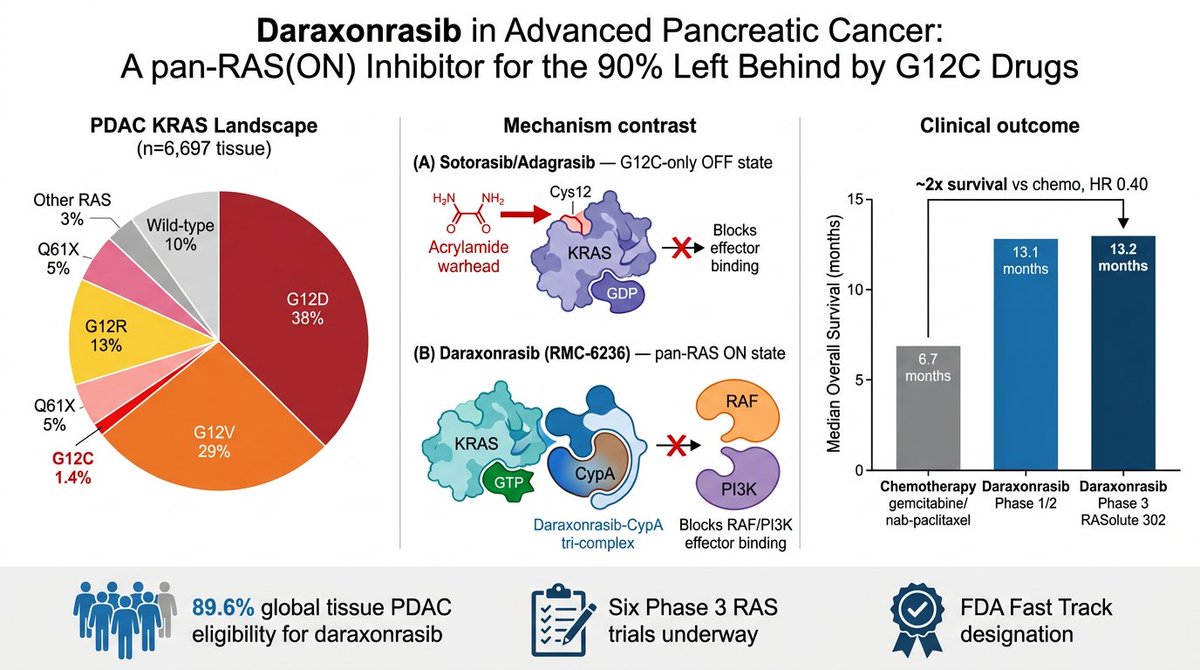
RAS finally getting drugged is one of the great stories in modern biology, and almost nobody outside oncology understands why it's such a big deal.
YOU'LL LEARN SOMETHING AWESOME TODAY.
i am going to keep this as understandable (and simple) as i can.
OPEN THE THREAD.
🧵
@DrJackKruse Hmm... Not sure about this being a conspiracy to keep the knowledge hidden by mainstream entomology or medicine.
Here's a very recent study on sulfur or copper particles: https://t.co/IOievQySbJ
TLDR - sulfur kills ticks as adults, larvae, or eggs.
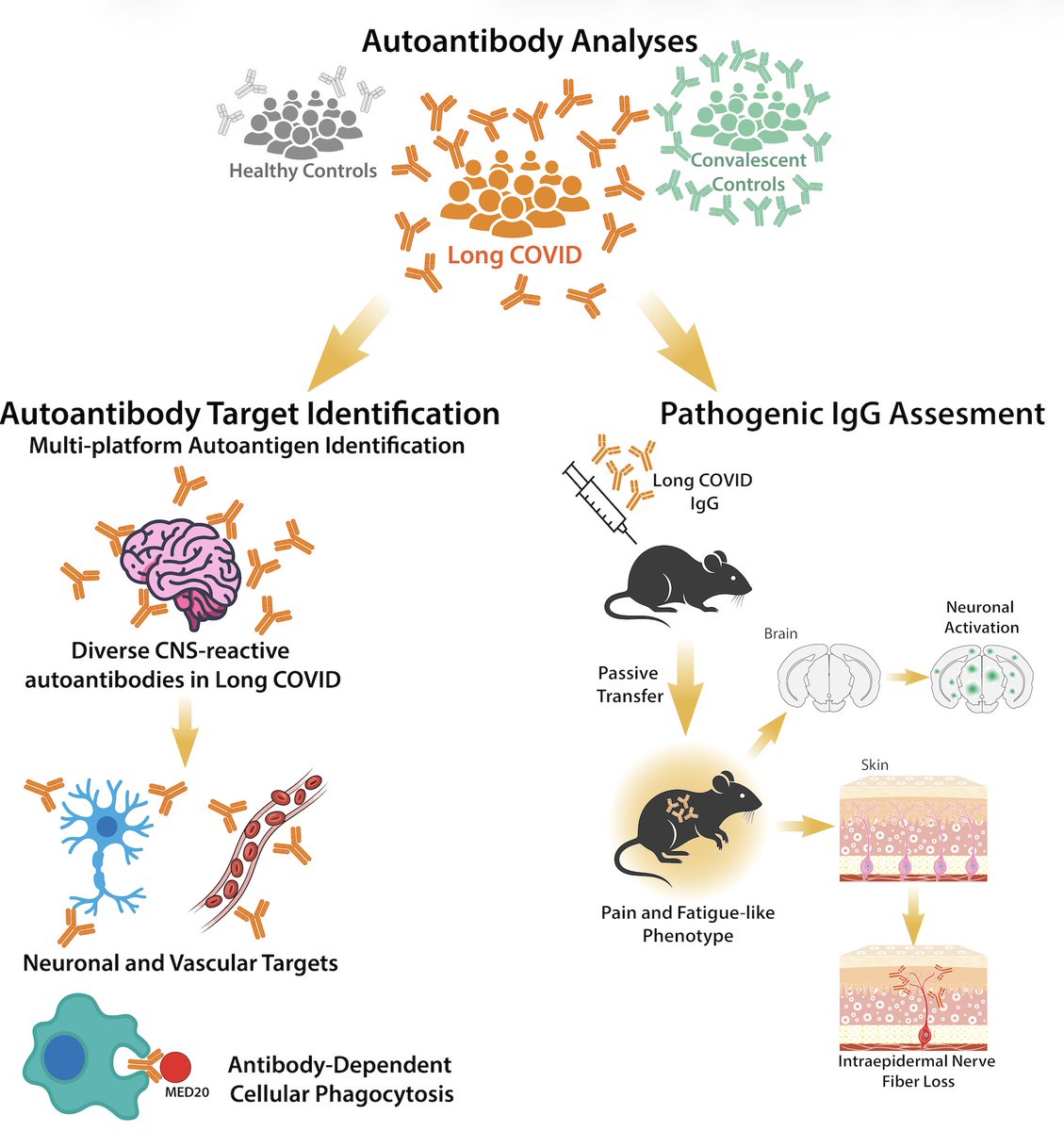
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
Ooohhhh.... This is an interesting study.
Researchers from the University of Arizona have developed a urine test for autism based on gut microbe metabolites. The test has 90% sensitivity and 100% specificity based on the metabolite levels in the urine.
For anyone interested in autism, it is worth reading through the introduction section (and the discussion at the end). The researchers go into the changes in the gut microbiome seen in the majority of people with autism, but then also touch on the ones without gut changes usually having rare genetic mutations that are driving the autistic symptoms.
Here's a few quotes that I thought were interesting:
"In the context of early neurodevelopment, abnormal elevation of certain microbial metabolites—particularly those derived from tryptophan and phenylalanine metabolism—has been associated with adverse effects on gut barrier function, immune signaling, neurotransmitter pathways, and neurobehavioral outcomes"
"Among participants with autism spectrum disorder (ASD), 42% exhibited high levels of one or more tryptophan metabolites, 57% had elevated phenylalanine/tyrosine metabolites, and 26% had high levels of both one tryptophan metabolite and one phenylalanine metabolite. 16% of ASD participants showed increased levels of yeast metabolites." 👇
Let me trace the timeline here because nobody's connecting it.
Step 1: Scrape the entire internet. Every book, every article, every conversation, every piece of art, every forum post. Do it without asking. Do it without paying.
Step 2: Train a model on all of it. Call it "artificial intelligence."
Step 3: Go to BlackRock's Infrastructure Summit and announce: "We see a future where intelligence is a utility, like electricity or water, and people buy it from us on a meter."
Step 3 is where you sell people's own knowledge back to them. On a meter.
They took the collective output of human thought, compressed it into a model, and now they want to charge you by the token to access a version of what you and everyone you know already created.
One Reddit user put it perfectly: "They stole all this data from us, the people, our life's work, creativity, art, by devouring the internet and blowing through all copyright laws. Now they want to sell it back to us in the form of a utility."
Imagine if someone photocopied every book in the public library, burned the library down, and then opened a subscription service for the copies.
That's the metered intelligence business model.
And they're pitching it to infrastructure investors as though they invented water.
Here’s another new study on long Covid and ME/CFS. The researchers looked at neurotransmitter levels in the brains - specifically the catecholamine system. They found reduced norepinephrine levels, compared to healthy controls, in people with post-infectious ME/CFS, long Covid, and Parkinson’s (the Parkinson’s patients were included as reference because they have known impairments in this pathway).
Interestingly, the ME/CFS and long Covid patients had no changes to dopamine levels, just norepinephrine. Dopamine is upstream of norepinephrine, and the DBH enzyme converts dopamine to norepinephrine.
Norepinephrine is produced mainly in the brainstem and regulates attention, focus, sleep cycles, and mood. It’s also involved in the regulation of breathing and hypoxia.
https://t.co/dePQYGzTuP
(And yes, I'm working on an article on genes involved in norepinephrine synthesis and transport)
Semaglutide reversed osteoarthritis damage in a new Cell Metabolism study—and the effect was independent of weight loss.
The drug reprogrammed how cartilage cells generate energy, enabling damaged cartilage to regenerate rather than just slowing degeneration.
Osteoarthritis has traditionally been treated as inevitable wear-and-tear. Existing therapies are palliative—NSAIDs reduce pain, hyaluronic acid injections provide temporary lubrication. Nothing clinically available has reversed cartilage loss.
The assumption with GLP-1 drugs was straightforward: weight loss reduces joint load, which protects cartilage. Less mechanical stress means less damage.
But this study included a pair-feeding control group where mice ate the same restricted amount as semaglutide-treated mice—producing comparable weight loss without receiving the drug.
The pair-fed mice lost weight but didn't get cartilage protection. Only semaglutide-treated mice showed reduced cartilage degeneration, fewer bone spurs, and decreased joint membrane inflammation.
This demonstrates a weight-loss-independent mechanism operating directly in cartilage tissue itself.
The molecular pathway: semaglutide activates what researchers call the GLP-1R-AMPK-PFKFB3 axis in chondrocytes—the specialized cells that produce and maintain the cartilage cushioning your joints.
When GLP-1 receptors are activated, they trigger AMPK—a cellular energy sensor that regulates metabolism. AMPK then suppresses PFKFB3, an enzyme that pushes cells toward a fast but inefficient energy production pathway called glycolysis.
By inhibiting PFKFB3, semaglutide forces chondrocytes to shift away from glycolysis and toward mitochondrial oxidative phosphorylation—a slower but far more efficient way to generate cellular energy.
Why this matters: In osteoarthritic joints with metabolic dysfunction, cartilage cells rely heavily on glycolysis to produce energy. Glycolysis is the metabolic pathway your muscles use during intense exercise when oxygen is limited—it's fast but produces only 2 ATP energy molecules per glucose and generates lactate as a byproduct.
Lactate accumulation worsens inflammation and creates an acidic environment that damages cartilage further.
Oxidative phosphorylation—the process that occurs inside mitochondria when oxygen is available—produces approximately 36 ATP molecules per glucose. It's 18 times more efficient and supports the long-term maintenance functions that cartilage cells need to survive and repair tissue.
When semaglutide shifts chondrocytes from glycolysis to oxidative phosphorylation, these cells become metabolically healthier and far more capable of surviving inflammatory stress while producing the structural proteins needed to maintain cartilage.
Researchers measured nearly 8,300 proteins in cartilage tissue and found coordinated changes in mitochondrial function, energy metabolism, and inflammatory signaling—all consistent with this fundamental metabolic shift.
The metabolic reprogramming translated to measurable outcomes. Semaglutide-treated mice showed reduced pain sensitivity, preserved cartilage structure, and decreased bone spur formation compared to controls.
A randomized human trial (ChiCTR2200066291) supported these preclinical findings. Participants receiving semaglutide showed greater improvements in WOMAC scores—a standardized questionnaire measuring osteoarthritis pain, stiffness, and physical function—compared to controls receiving only hyaluronic acid injections.
The most striking finding: cartilage thickness increased in the semaglutide group on imaging. Not just slower degeneration—actual regeneration of cartilage that had been lost.
Limitations exist. The human trial was small and cartilage assessments were unblinded, meaning evaluators knew which patients received semaglutide. The study focused specifically on metabolic osteoarthritis—the subtype driven by obesity, insulin resistance, and systemic metabolic dysfunction.
This mechanism may not generalize to all forms of osteoarthritis. Age-related wear, post-traumatic damage from injuries, or genetic forms may not respond the same way because the underlying pathophysiology isn't primarily metabolic.
But metabolic osteoarthritis represents a large and growing proportion of cases, especially in adults aged 30-44. The overlap with populations already prescribed GLP-1 drugs for diabetes or obesity is significant.
Semaglutide isn't correcting joint mechanics through weight loss. It's correcting the fundamental energy metabolism problem in damaged cartilage cells—restoring their mitochondrial function and enabling them to produce the collagen and glycosaminoglycans (complex sugars that form cartilage's gel-like cushioning structure) needed to maintain healthy tissue.
The intervention window likely exists before cartilage damage becomes irreversible. Once chondrocytes are dead and cartilage architecture is fully degraded, metabolic reprogramming can't restore what no longer exists.
But in early metabolic osteoarthritis—when cartilage cells are metabolically stressed but still viable—restoring oxidative phosphorylation capacity may prevent progression and reverse early damage.
The decisions made in the fourth and fifth decades about metabolic health—obesity, insulin resistance, chronic inflammation—may determine whether osteoarthritis becomes disabling in the sixth and seventh decades.
Semaglutide appears to offer a pharmacological tool to intervene on that trajectory by addressing the underlying metabolic dysfunction in cartilage tissue itself—not just reducing symptoms but correcting the cellular energy crisis that drives cartilage breakdown.
Is there an association between human herpesviruses (HHVs) reactivation and Long COVID? We analyzed HHV DNA shedding in saliva and found that HHV-6 correlates with Long COVID severity. Claire Laxton, @S_Tabachnikova, Lily Cooke, Kexin Wang et al.
https://t.co/jsZznyXiGq (1/)
“It Takes an Average of 17 Years for Evidence to Change Practice—the Burgeoning Field of Implementation Science Seeks to Speed Things Up.” Published April 5, 2023, JAMA. https://t.co/79WAxa55Vi
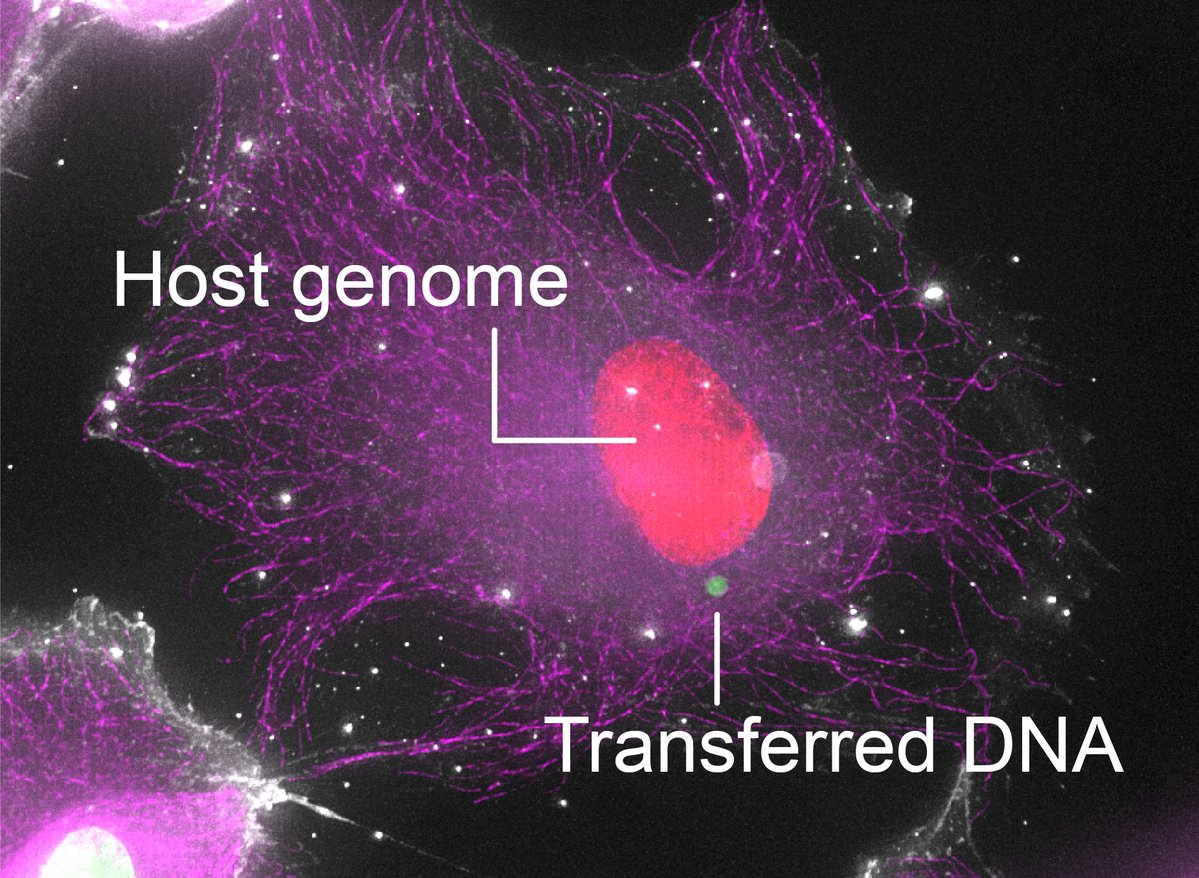
Excited to share our latest paper, out today @CellCellPress. We found that large pieces of the human genome can transfer between cells upon direct contact, endowing recipient cells with heritable phenotypic changes. (1/7)
https://t.co/SbshGhofN0