@sri_srikrishna@masknerd (Scores vary a lot depending on environmental conditions - the same mask might score much lower when tested with air that has more particles close to MPPS. Which corroborates the point that filtration efficiency depends on particle size - but I've never seen anything below 99%.)
@sri_srikrishna@masknerd This is also quite apparent when testing masks with a Portacount, or other CPC: N95s can achieve scores > 1000, equivalent to 99.9% exposure reduction - which implies that filtration efficiency is at least that high during the test.
@JonJonAnimation@ghhughes Perhaps modern half-face elastomerics are better under real world conditions, but no one appears to be doing these kinds of studies anymore...
@JonJonAnimation@ghhughes Full-face or half-face? Half-face P100 would be the exact same based on all available evidence (cf. APF from OSHA and other bodies, derived from WPF studies, etc.). The limiting factor is seal, not filtration.
(This infographic is using APF, and all half-face masks have APF=10.)
@mkarolian@CriticalAerosol Exposure reduction is typically significant, but not infinite. And overpromising can be dangerous - we've already seen how that worked out for other mitigations...
@mkarolian@CriticalAerosol What's your definition of "well fitted"; how many people actually achieve it? Is it the 1% penetration on the chart?
I'm guessing the author took 1% from a passing fit test score: few people realise this doesn't map directly to real life protection (or WPF) for a host of reasons
@AlexCurlew@snowleopardess@Nucleocapsoid@UKHSA I couldn't find anything about longer term harms so far, but... AFAIUI there's little to no data on seasonal boosters' influence on this, which could make it difficult to factor that into their models?
(They appear to be very focused on available evidence...)
@AlexCurlew@snowleopardess@Nucleocapsoid@UKHSA Yes and no: (disclaimer: I've only looked at some minutes) for higher risk people they seem to focus on hospitalisation and deaths. But they do consider protection against onward transmission for HCW (low), and also the challenges from waning protection + lack of seasonality.
@snowleopardess@Nucleocapsoid@UKHSA TL;DR: although the end result sucks, it's not arbitrary. It's all down to healthcare budgets, and manufacturer pricing at the end of the day.
@snowleopardess@Nucleocapsoid@UKHSA The reason that the advice changed this year is because they were previously using a different ("non-standard") cost-effectiveness model.
So the problem is either with their model (I haven't dug into that yet), or the pricing (which they have no influence over).
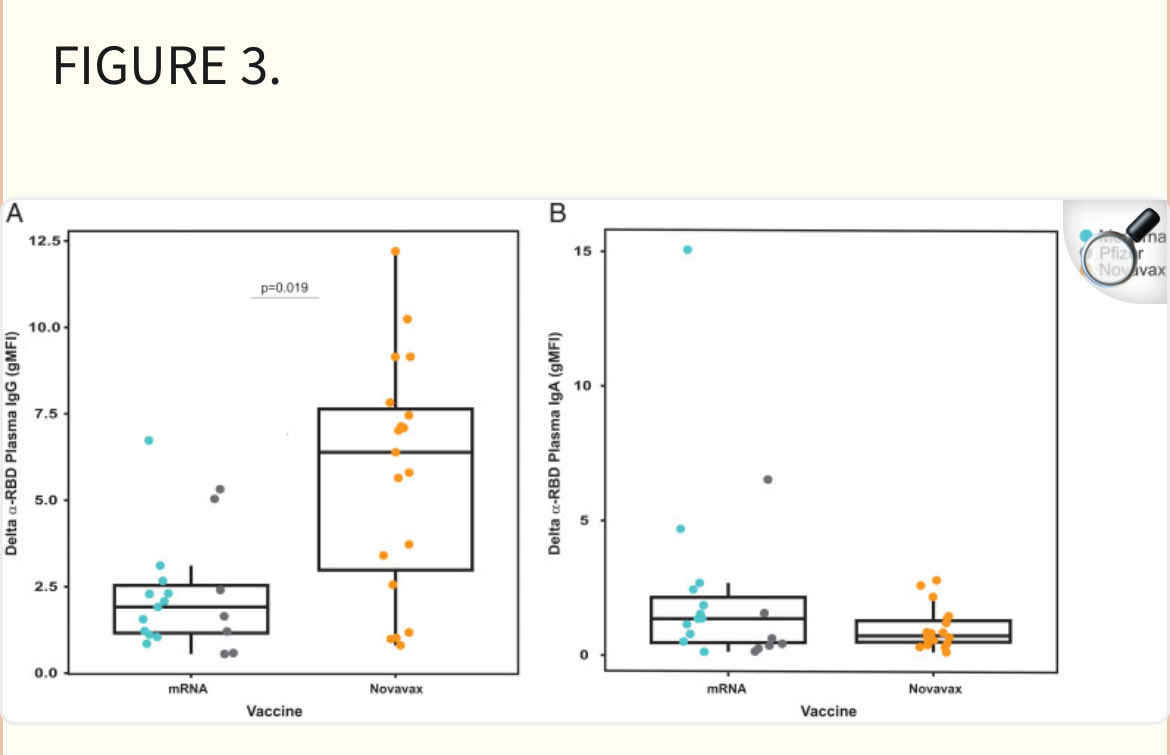
@JUurinmaki@jual1977 Based on n=19 per technology, with huge confidence intervals, and only for IgG (opposite for IgA).
Grouping Comirnaty and Spikevax also seems odd to me.
Hmm...
@SGriffin_Lab@_CatintheHat The price difference seems to be a much likelier explanation?
~10x higher price for Covid Vax -> much higher cost/QALY (or whatever metric they use)?
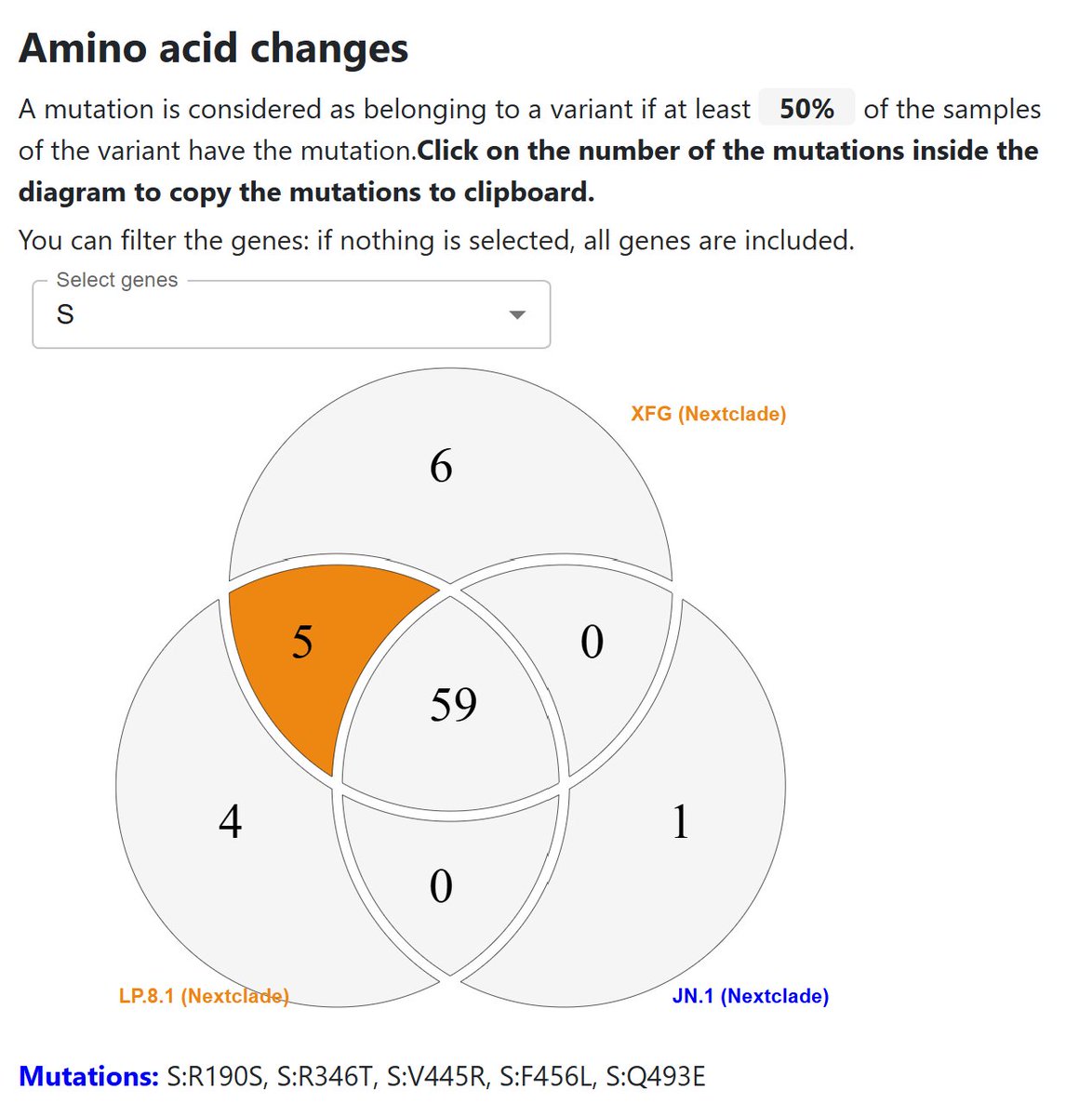
@SGriffin_Lab Here's another version comparing JN.1, LP.8.1 and XFG, for those of us who are still only offered a JN.1 vaccine, which is missing even more important escape mutations.
2/
Does the original PortaCount 8020 (non-A) not support external control?
This specimen does send data in test and count modes per usual, but ignores any requests to switch to external control.
The appropriate pins do appear to be connected, most importantly 3 (RX).
They wouldn't put the external control indicator on this machine if it wasn't supposed to work, right?