The #1 question I get from patients on Wegovy and Zepbound:
"Do I have to take this forever?"
The honest answer used to be yes.
New data says it's more nuanced than that. I break it all down here:
https://t.co/j1Djn3McMZ
Subscribe for more evidence-based deep dives → https://t.co/pAVWtSE5PV
#SubstanceOverNoise
⚖️💊 What happens when weight-loss drugs stop? The uncomfortable truth
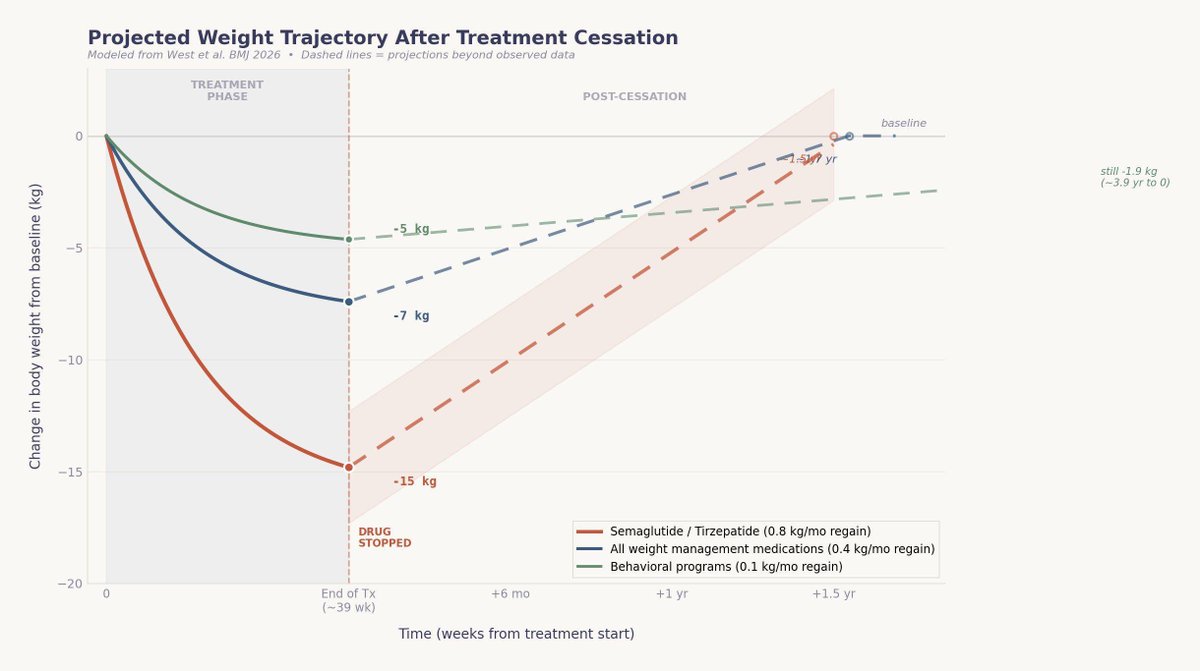
This 2026 BMJ systematic review and meta-analysis delivers one of the clearest reality checks yet on weight regain after stopping weight-management medications (WMMs), including GLP-1 and dual incretin therapies .
🔍 What was studied
Across 37 studies (63 treatment arms, 9,341 adults) with overweight or obesity, the authors quantified how fast weight returns after discontinuing medication, and compared this with regain after behavioural weight-management programmes (BWMPs). Follow-up extended up to two years after treatment cessation.
📉 The headline finding
On average, people regain 0.4 kg per month after stopping WMMs. At this pace, baseline weight is reached again within ~1.7 years.
For newer, highly effective incretin drugs (e.g. semaglutide, tirzepatide), regain is even faster—up to 0.8 kg/month, with return to baseline in ~1.5 years.
🫀 Metabolic benefits fade too
Improvements in HbA1c, fasting glucose, lipids, and blood pressure closely track weight. Once medication stops, cardiometabolic markers steadily worsen, returning to baseline within ~1.4 years. Weight loss without maintenance = temporary risk reduction.
⚠️ Worse than lifestyle alone
When directly compared, weight regain after stopping drugs was significantly faster than after stopping behavioural programmes, independent of how much weight was initially lost. Bigger losses tended to rebound faster—biology pushes back hard.
🧠 Why this matters
Obesity behaves like a chronic, relapsing disease. Short-term pharmacotherapy without a long-term plan risks disappointment, lost benefit, and misaligned expectations—for patients and health systems alike.
🔮 Bottom line
Weight-loss drugs are powerful—but they don’t “cure” obesity. Their benefits persist only while treatment continues, or if embedded in a sustained, comprehensive strategy.
Stopping therapy doesn’t just pause progress—it reverses it 🚨
Obesity remains one of the UK’s most complex and urgent public health challenges with profound social and economic consequences.
A new report developed by Brightsparks Agency explores the human, social, and financial impact of obesity.
Read more: https://t.co/IUdXO4U2xx
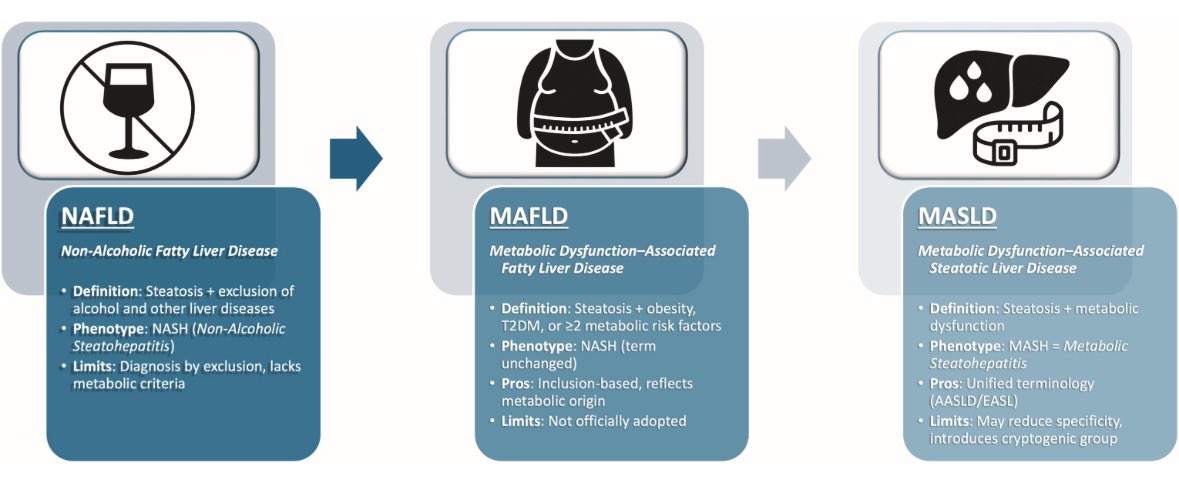
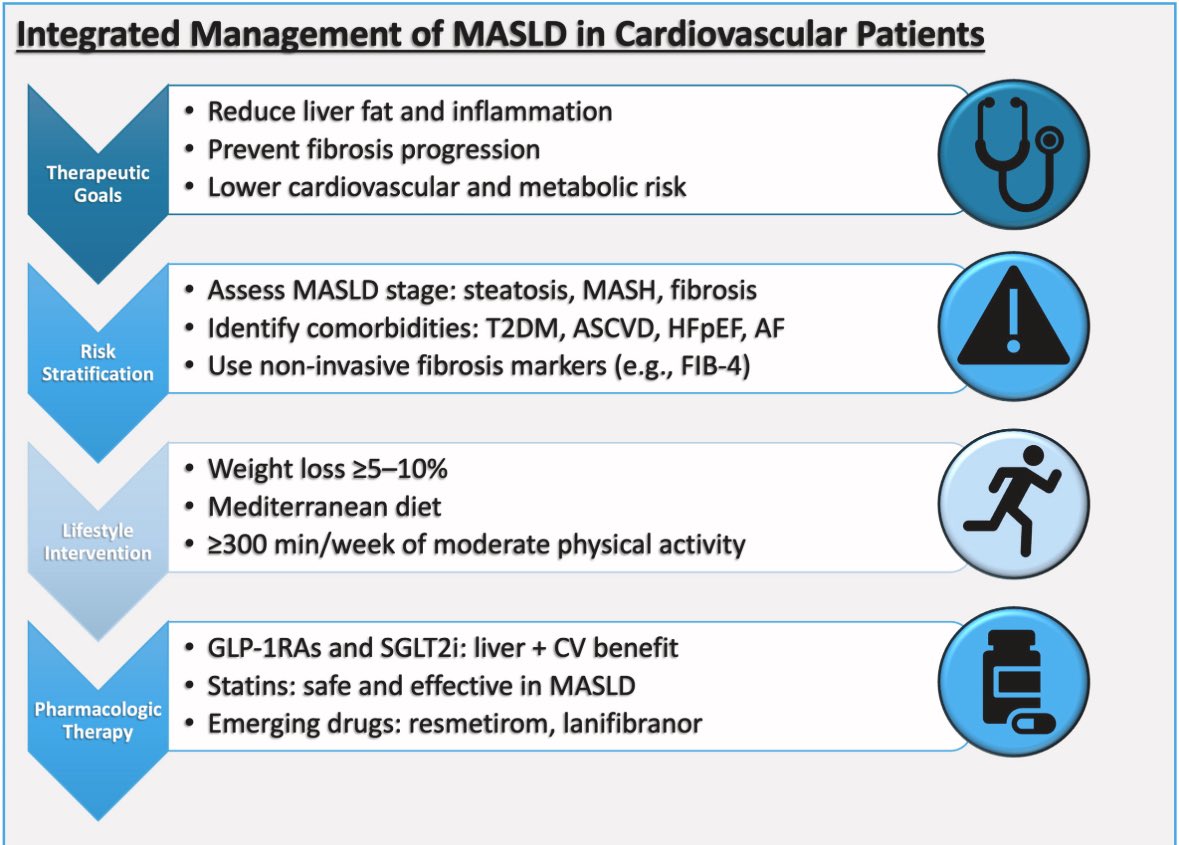
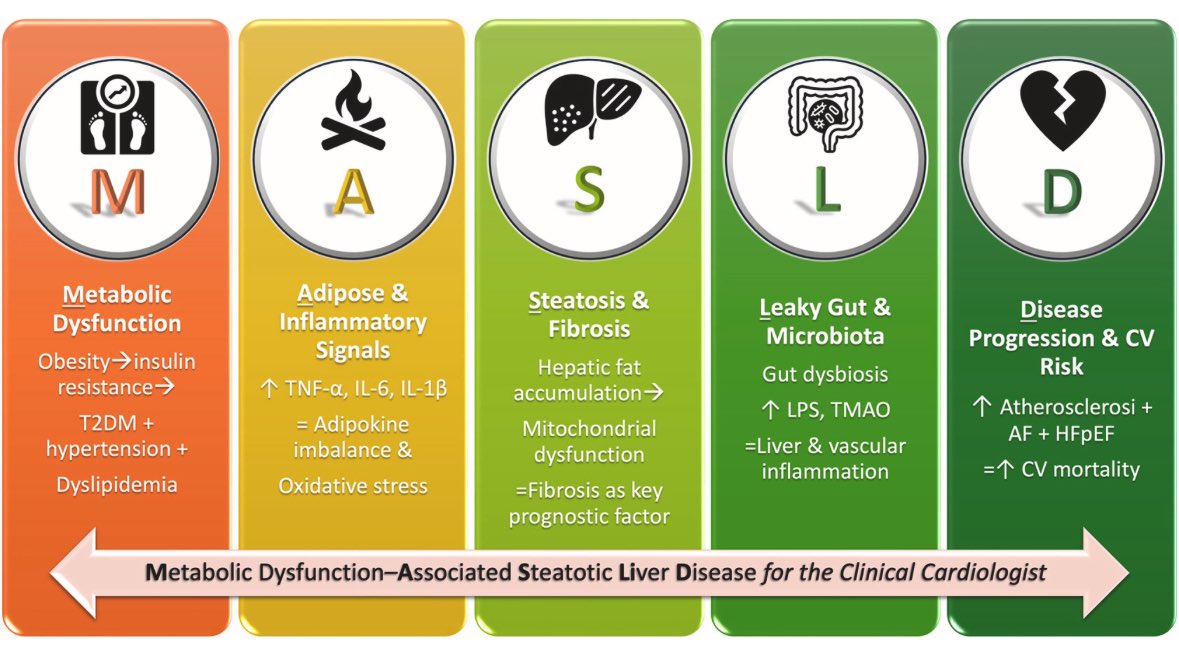
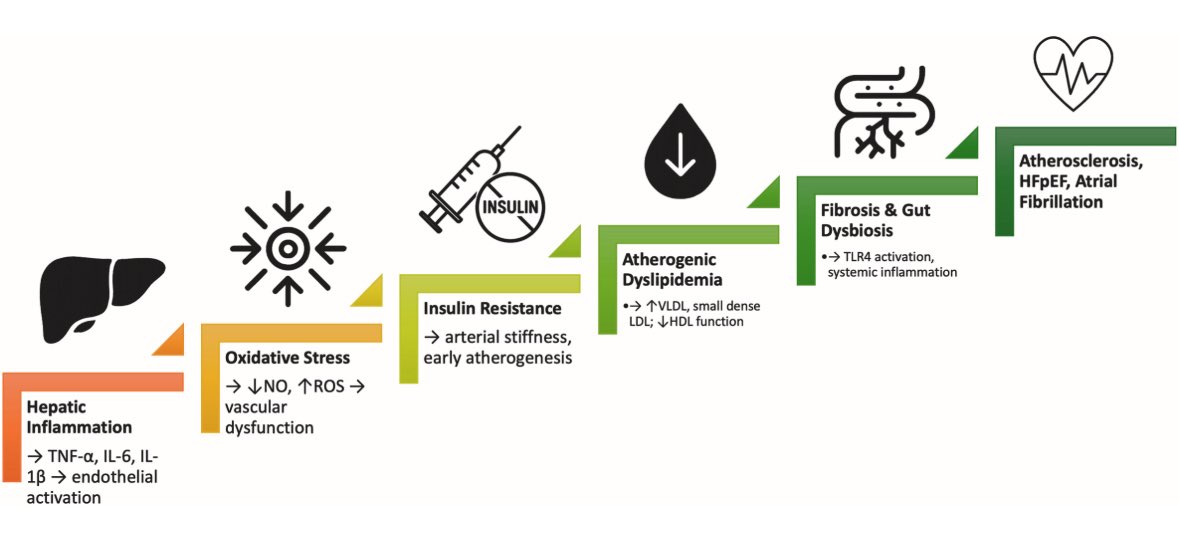
👉Understanding MASLD — from molecular pathogenesis to cardiovascular risk:
A concise review for the clinical cardiologist
MASLD not only drives liver injury but also worsens lipid metabolism, fueling atherogenic dyslipidemia: ↑ VLDL, small dense LDL, dysfunctional HDL.
The review in @ATHjournal highlights that:
•Statins are both safe and effective in MASLD, yet underprescribed.
•Ezetimibe and pemafibrate may improve lipid profile and hepatic parameters.
•GLP-1RAs and SGLT2i show dual benefit on liver fat, cardiometabolic risk, and CVD outcomes.
•Emerging agents (resmetirom, lanifibranor) target both hepatic fibrosis and lipid metabolism.
☝️Take-home: lipid-lowering therapy remains central in MASLD management, but must be integrated with newer agents for optimal cardio-hepatic protection .
🔗 https://t.co/pLoCWwpr5D
@society_eas
Bariatric Surgery vs GLP-1 @JAMASurgery
• 30,458 pts insurance database in the US -2yr f/u
• Bariatric surgery better weight loss
(28.3% vs 10.3%)
• Bariatric Surgery saving $11 689 in ongoing costs
doi: 10.1001/jamasurg.2025.3590
@ASMBS@IfsoSecretariat@IFSO_NAC@frankman1987
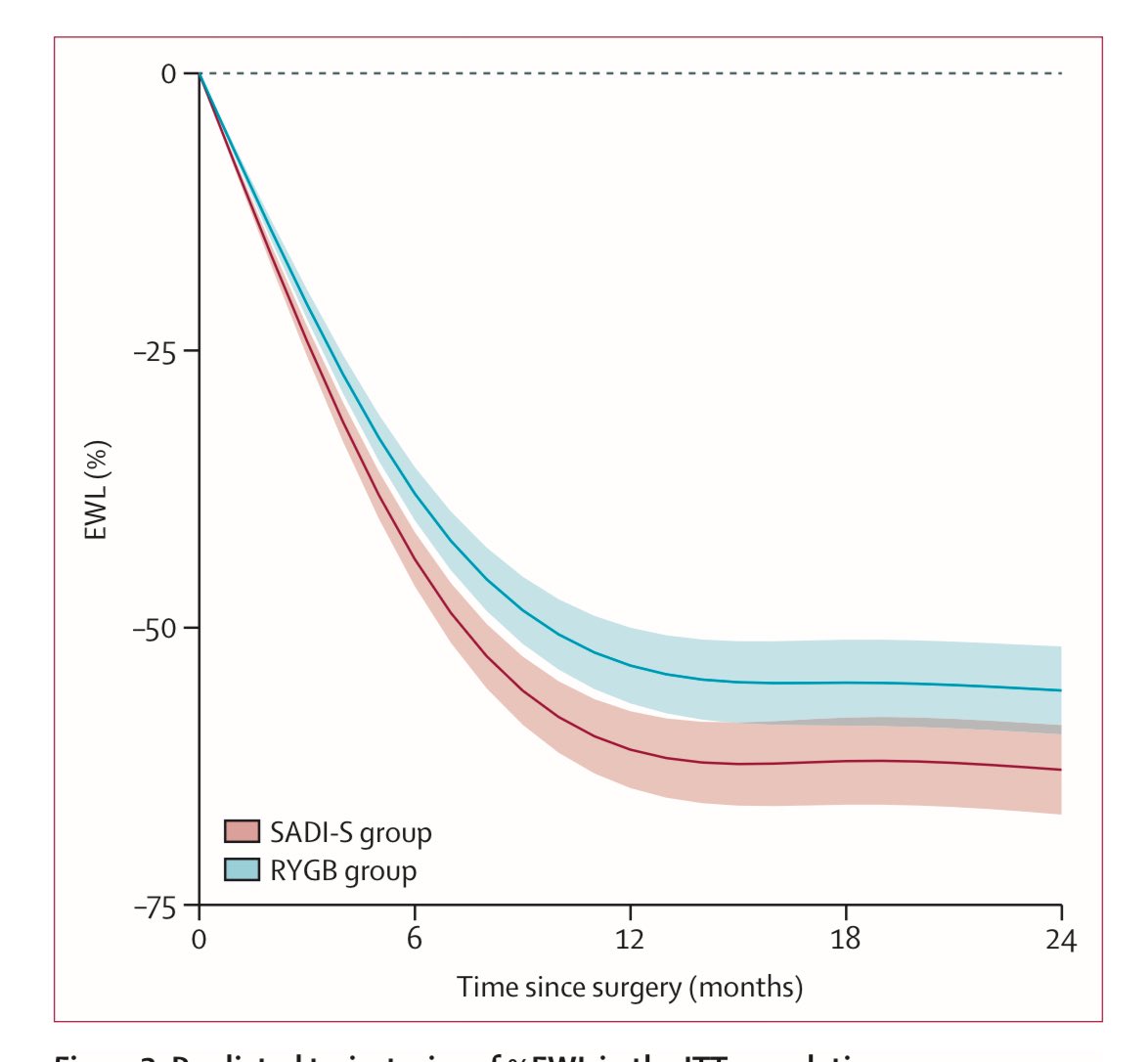
SADISLEEVE RCT published 2yr multi center in France @TheLancet
%TWL:
–33·3% SADI-S group vs
–30·2% RYGB group and
%EBL: –76·1% vs –68·6 respectively (p=0·018)
• Metabolic benefits: Comparable diabetes and hypertension remission.
• Safety: Early safety similar (Leaks SADI=3 vs RNY=1), but SADI-S had fewer late complications and fewer reoperations (Internal hernias: SADI=0 vs RNY=5)
• Nutritional risk: Slightly higher with SADI-S (more fat-soluble vitamin deficiencies D, E, A, folate and higher diarrhea and steatorrhea rates)
https://t.co/IxNfgRO4XV
@ASMBS@IfsoSecretariat@IFSO_NAC
📉 What REALLY happens when you stop anti‑obesity meds?
- - -
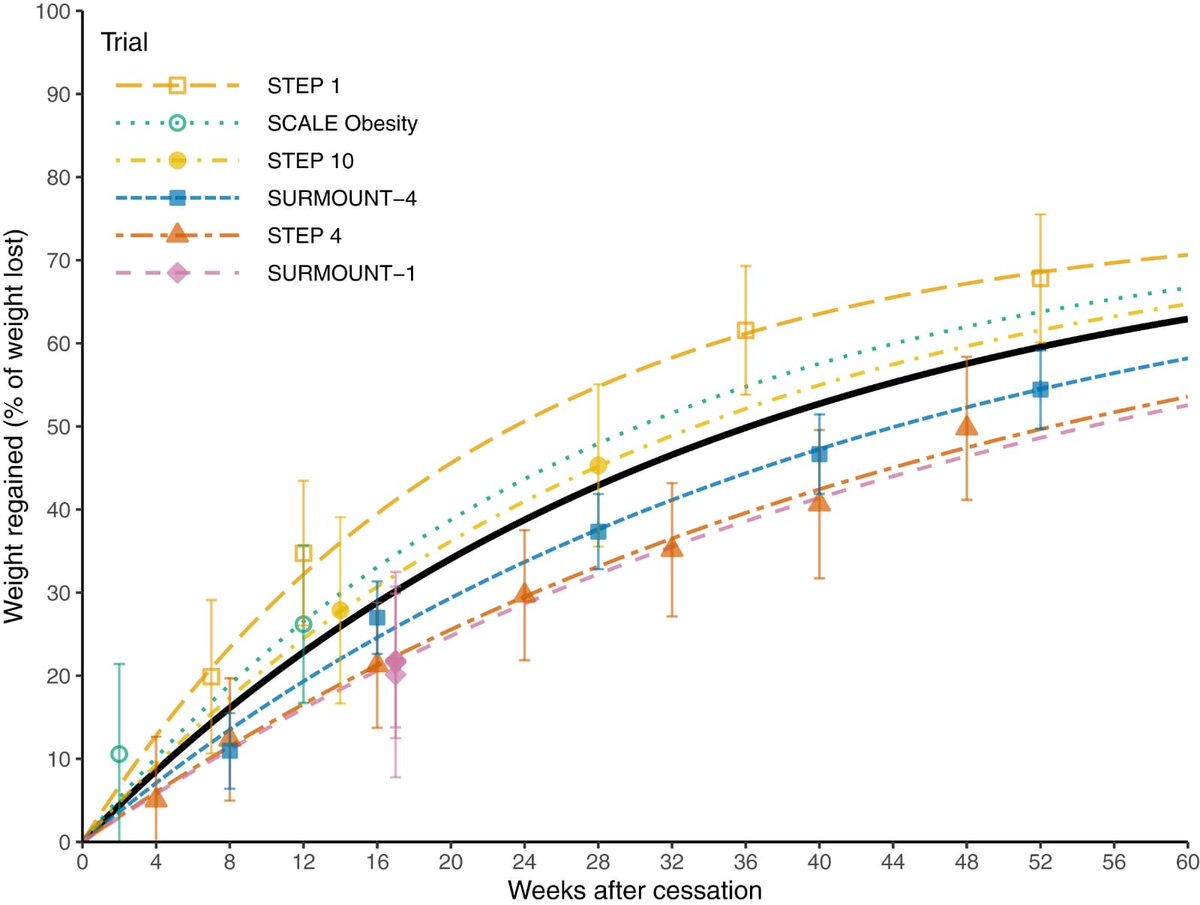
A new meta‑analysis [Wu et al., BMC Medicine, 2025] just mapped the weight regain trajectory after stopping GLP‑1s and other AOMs—and it’s eye‑opening.
Key findings:
⏳ First month off: Weight loss continues briefly (~4 weeks).
📈 By week 8: Regain starts.
🔄 Weeks 8–20: Rapid regain — often 2–3 kg above discontinuation weight.
🪂 After ~6 months: Regain levels off, but most patients keep some net loss vs. baseline.
💉 GLP‑1s hit harder: GLP‑1–based drugs showed the most pronounced regain.
🏋️♀️ Lifestyle changes help… but not enough: Even with ongoing diet/exercise programs, regain still occurred.
Why?
🔹Appetite & hunger hormones rebound.
🔹Stomach emptying speeds back up.
🔹Metabolic rate adjusts downward after weight loss.
The takeaway:
Stopping AOMs ≠ “you’re cured.” Obesity is a chronic condition — and without ongoing treatment (whether medication, surgery, or intensive behavioral support), biology will try to pull weight back up.
🔗https://t.co/fP6jHaY91i
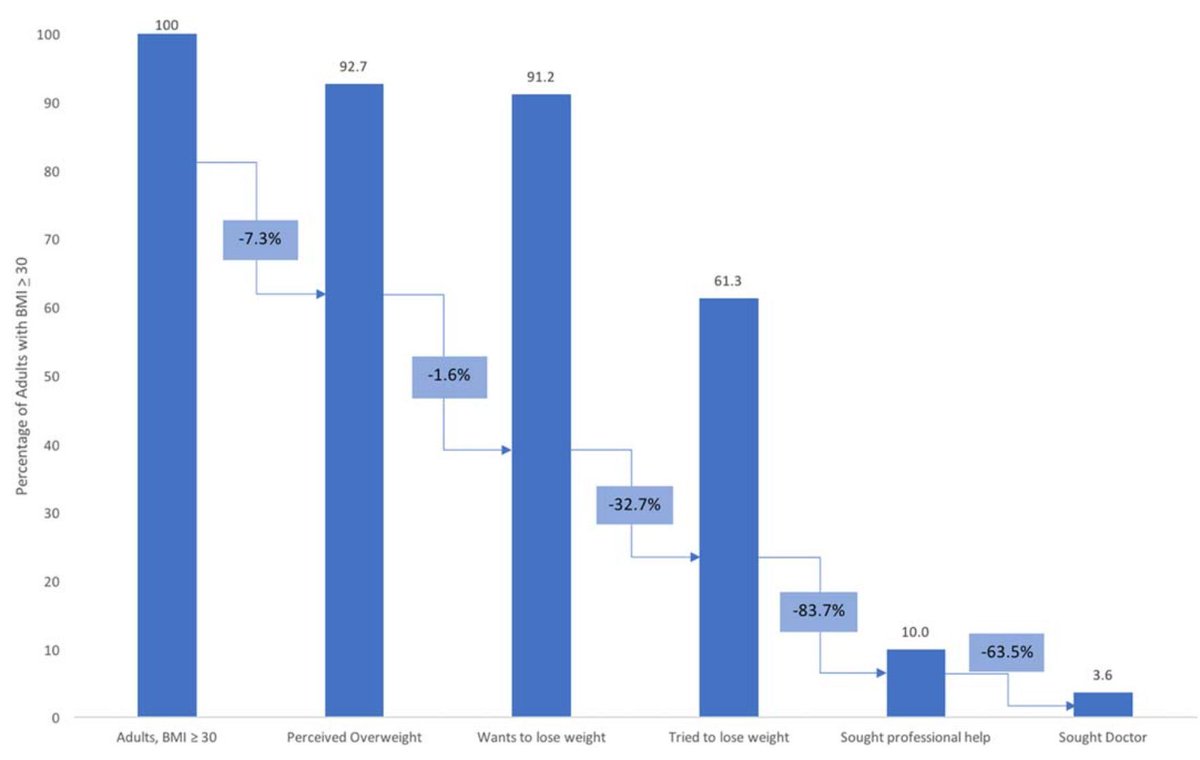
📊 The Obesity Care Cascade 🏥
Where does the breakdown occur in those who have BMI >30 and those who seek a doctor for advice? 🤔
🔻 The largest drop-off (83.7% relative disengagement) occurred between trying to lose weight and seeking professional help 💔
🔻 The second largest gap (63.5% disengagement) was between seeking any health professional versus seeking physician care specifically 👩⚕️➡️👨⚕️
https://t.co/LhfNEJBDDI















![MichaelAlbertMD's tweet photo. 📉 What REALLY happens when you stop anti‑obesity meds?
- - -
A new meta‑analysis [Wu et al., BMC Medicine, 2025] just mapped the weight regain trajectory after stopping GLP‑1s and other AOMs—and it’s eye‑opening.
Key findings:
⏳ First month off: Weight loss continues briefly (~4 weeks).
📈 By week 8: Regain starts.
🔄 Weeks 8–20: Rapid regain — often 2–3 kg above discontinuation weight.
🪂 After ~6 months: Regain levels off, but most patients keep some net loss vs. baseline.
💉 GLP‑1s hit harder: GLP‑1–based drugs showed the most pronounced regain.
🏋️♀️ Lifestyle changes help… but not enough: Even with ongoing diet/exercise programs, regain still occurred.
Why?
🔹Appetite & hunger hormones rebound.
🔹Stomach emptying speeds back up.
🔹Metabolic rate adjusts downward after weight loss.
The takeaway:
Stopping AOMs ≠ “you’re cured.” Obesity is a chronic condition — and without ongoing treatment (whether medication, surgery, or intensive behavioral support), biology will try to pull weight back up.
🔗https://t.co/fP6jHaY91i](https://pbs.twimg.com/media/GxO5a4LW0AAn5_j.jpg)























![MichaelAlbertMD's tweet photo. 📉 What REALLY happens when you stop anti‑obesity meds?
- - -
A new meta‑analysis [Wu et al., BMC Medicine, 2025] just mapped the weight regain trajectory after stopping GLP‑1s and other AOMs—and it’s eye‑opening.
Key findings:
⏳ First month off: Weight loss continues briefly (~4 weeks).
📈 By week 8: Regain starts.
🔄 Weeks 8–20: Rapid regain — often 2–3 kg above discontinuation weight.
🪂 After ~6 months: Regain levels off, but most patients keep some net loss vs. baseline.
💉 GLP‑1s hit harder: GLP‑1–based drugs showed the most pronounced regain.
🏋️♀️ Lifestyle changes help… but not enough: Even with ongoing diet/exercise programs, regain still occurred.
Why?
🔹Appetite & hunger hormones rebound.
🔹Stomach emptying speeds back up.
🔹Metabolic rate adjusts downward after weight loss.
The takeaway:
Stopping AOMs ≠ “you’re cured.” Obesity is a chronic condition — and without ongoing treatment (whether medication, surgery, or intensive behavioral support), biology will try to pull weight back up.
🔗https://t.co/fP6jHaY91i](https://pbs.twimg.com/media/GxO5a7AW4AIXPAG.jpg)