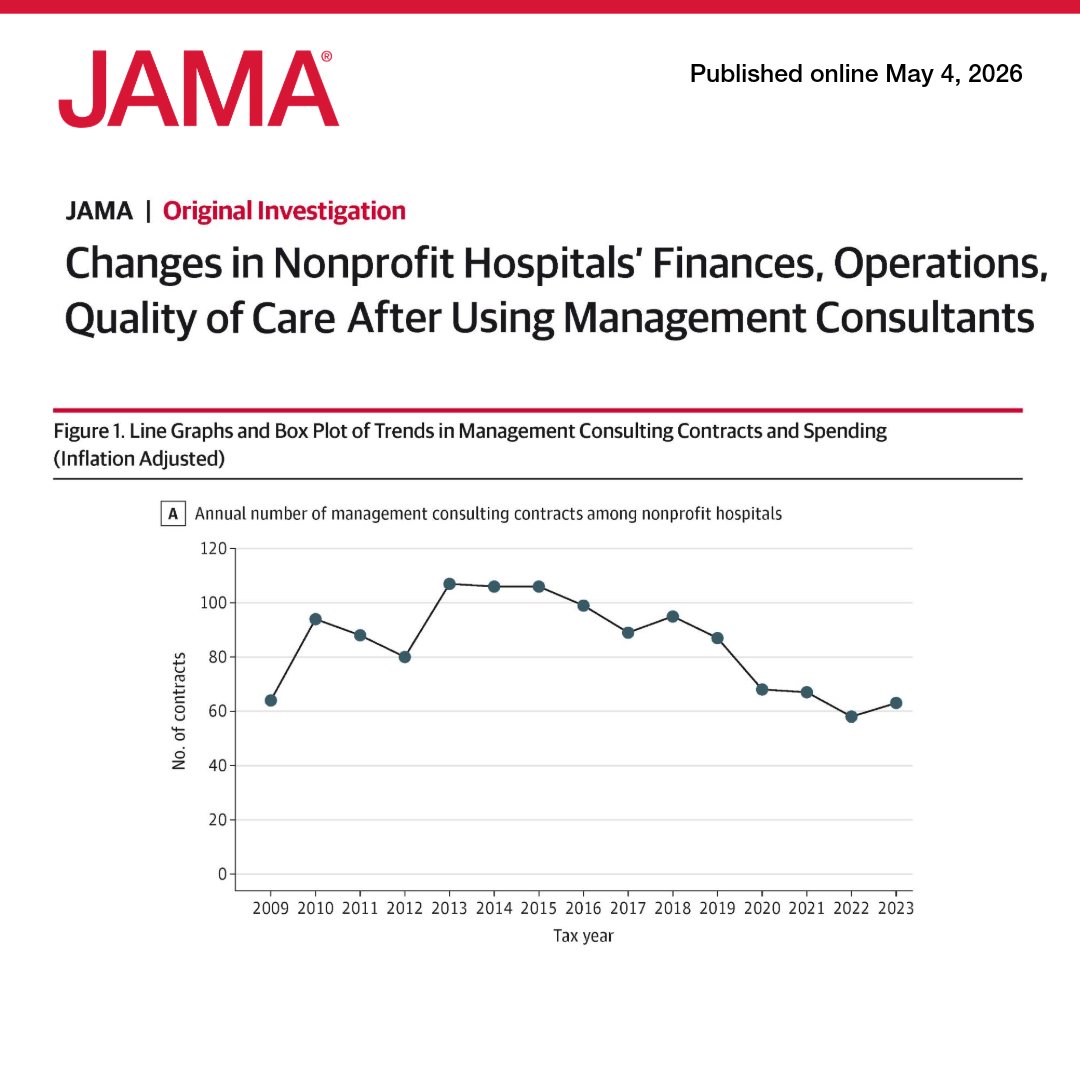
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8
One of the most expensive mistakes a man can make is to carry responsibility without carrying authority, because once you are expected to absorb pressure without being able to shape outcomes, you stop becoming valuable and start becoming convenient to exploit for other people’s comfort.
Hospitals have convinced a generation of doctors that the building is the value.
(Funny how that theory disappears the second there is a lawsuit)
Without doctors: no admissions, no surgeries, no procedures, no E&M billing, no facility fees, no DRGs, no MCC/CC capture, no 340B scripts, no quality metrics.
The building collects the fee.
The doctor creates the value.
That is the relationship. Time physicians started acting like it.
Thanks for being a poster judge at the symposium, @InkedHeartDoc.
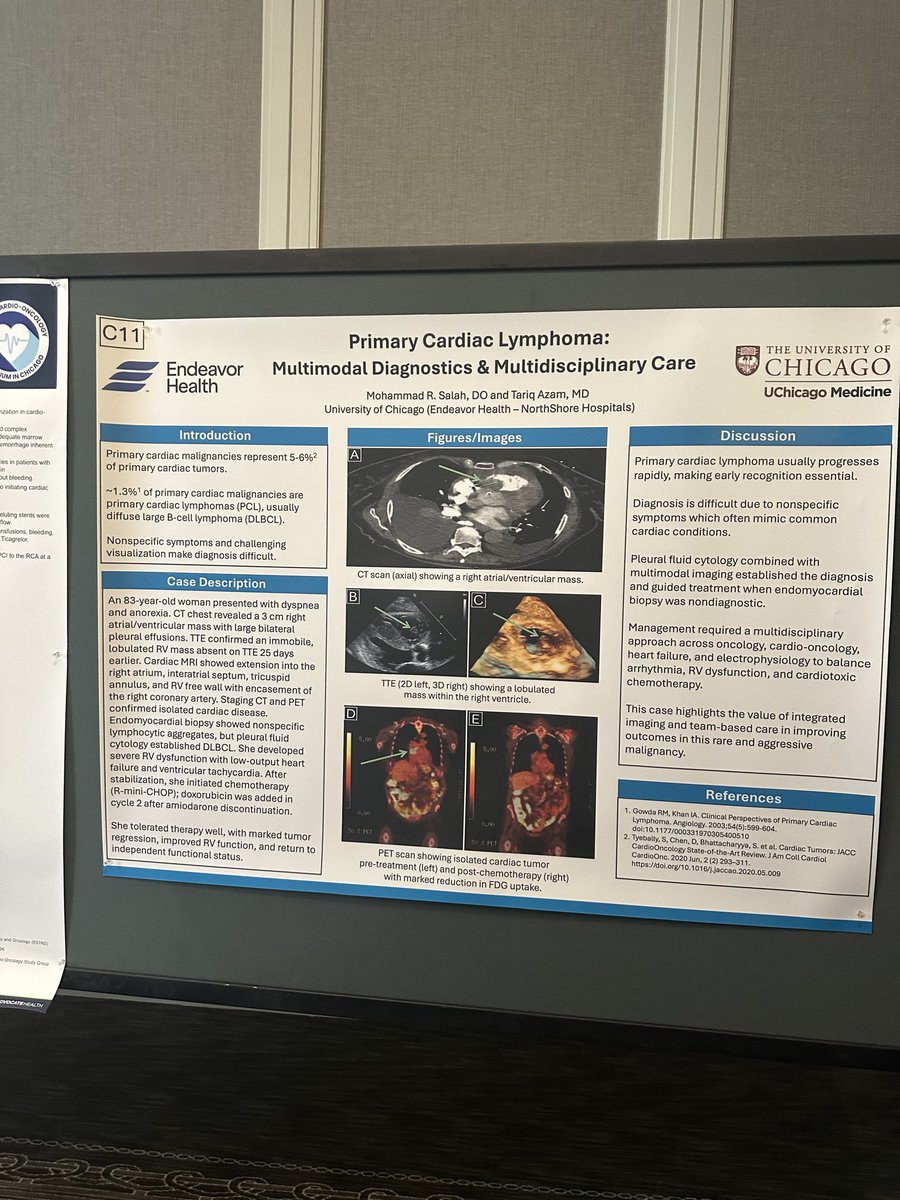
The #Midwest#CardioOncology Symposium in #Chicago was a wonderful success! With over 100 attendees and 24 posters—plus even more abstracts submitted—it was a vibrant day of learning, networking, and idea exchange. Students, trainees, and attendees left energized, better equipped to care for #patients and move forward in their careers. That was the heart of our mission.
#CardioTwitter #MedTwitter #MedEd #Cardiology #Oncology #Pharmacy #Medicine
Great to meet such a great cardio-onc group during the regional Cardio-onc symposium on current paradigms in CV care of cancer patients and survivors
#cardiotwitter#CardioOnc
✨ Exciting day at @CookCountyHealth! Starting fellowship interviews for the next generation of cardiologists. Grateful to be part of the recruitment committee and to meet the brilliant minds shaping the future of cardiovascular care. ❤️🫀 #Cardiology#MedTwitter#Fellowship
NPO before elective cath lab? Data say rethink it.
1/ SCOFF RCT (Eur Heart J 2024, n=716): primary safety composite 12.0% (no-fast) vs 19.1% (fast) → non-inferior & superior, with higher patient satisfaction.
2/ TONIC (JACC:CI 2024, n=739): ad-lib food/drink vs standard fasting before coronary procedures → primary composite 8.2% vs 9.9% = non-inferior; less hunger/thirst. No food-related adverse events.
3/ CALORI (JSCAI 2024, n=198): liberal oral intake up to the procedure vs NPO after midnight → better well-being & satisfaction, no safety penalty (no ↑ emesis/aspiration/intubation).
4/ AJCC 2024 RCT (n=197): heart-healthy diet allowed vs NPO before elective cath → no safety signal, satisfaction ↑; thirst/hunger ↓.
5/ 📌 Big picture: Across multiple RCTs, routine NPO for elective cath under conscious sedation isn’t supported—comfort improves, safety is comparable or better with non-fasting.
Time to modernize protocols. 💬 What’s your lab doing?
#CardioTwitter #FOAMed
This will be absolutely devastating in the medical field.
~30% residents are international medical graduates & ~10k of 43k residency spots are filled by docs with H1-B visas.
Previously the h-1B fee was <$5,000.
No hospital will pay a $100k fee for a $55k resident salary.