Bila bercakap tentang masyarakat India, kebiasaannya perbincangan akan tertumpu kepada berapa banyak program khas yang diumumkan, berapa ramai menteri India yang dilantik, atau agensi mana yang diwujudkan untuk menjaga kepentingan komuniti itu.
Saya faham kenapa pendekatan itu popular. Tetapi saya juga rasa sudah sampai masanya kita bercakap secara jujur tentang sama ada pendekatan itu benar-benar menyelesaikan masalah.
Pandangan saya mungkin tidak disenangi semua pihak.
Kita kena ubah budaya yang menyebabkan rakyat terpaksa "memohon". Sepatutnya, kalau dah benar-benar susah, golongan ini patut secara automatik mendapat bantuan.
Seorang keluarga India yang miskin tidak sepatutnya memerlukan program khas untuk membuktikan mereka layak dibantu. Begitu juga keluarga Cina yang miskin, keluarga Melayu yang miskin, atau mana-mana rakyat yang sedang bergelut untuk meneruskan kehidupan.
Fokus kerajaan sepatutnya bukan kepada siapa yang paling kuat mendakwa mewakili sesuatu kaum.
Fokus kerajaan mesti kepada siapa yang memerlukan bantuan dan memastikan mereka benar-benar menerima bantuan itu.
Mudah untuk mengatakan dasar perlu berasaskan keperluan. Ramai yang pernah mengatakannya. Cabaran sebenar ialah pelaksanaannya.
Sebab itu saya percaya kerajaan perlu berani menjawab satu soalan yang sering dielakkan: apakah sebenarnya yang dimaksudkan dengan "berasaskan keperluan"?
Apakah ukurannya? Siapa yang layak? Bagaimana kita memastikan bantuan sampai kepada mereka yang memerlukan, tanpa mengira kaum?
Kita perlu berani mengadakan perbincangan ini secara terbuka dan jujur dan mencari cara baru untuk memastikan rakyat yang benar-benar memerlukan menerima bantuan.
Pada akhirnya, rakyat tidak peduli siapa mendapat kredit politik kerana mereka mahu tahu sama ada kehidupan mereka menjadi lebih baik.
“Doctors are the worst patients,” they say.
I don’t know whether we are the worst patients, but we are definitely not the smartest ones.
A senior and respected doctor from a nearby town had central chest pain about 5 days ago. He dismissed it as “gastritis ” and continued running his busy OPD.
The next day, he developed chest pain again while working out in the gym, but ignored it thinking it was due to lifting weights.
The pain continued over the next few days, and by the 4th day he was unable to operate.
That evening he finally came to us.
His ECG showed an evolved anterior wall MI ,( a major heart attack). Echo showed an LV EF of just 35%. He had already developed Q waves.
Since he still had ongoing chest pain, we took him up for coronary angiogram , which showed a subtotal occlusion of the LAD ,( “widow maker.”)
He underwent successful angioplasty and went home
But this part hit me hard
As his wife , (herself a doctor) was taking him to the ER, patients waiting outside started arguing with her because he was leaving without finishing the OPD.
She literally had to plead with them, saying: “He is probably having a heart attack… he will see you if he comes back alive.”
And the last thing this poor doctor asked me before discharge was: “Can I restart OPD in 3–4 days?” 🤦
I’m sure this is the story of many of us in medicine.
We ignore our health and behave as though we are indispensable.
Many cardiologists have succumbed ignoring chest pain. I m sure colleagues on #MedTwitter and #CardioTwitter would have similar experiences !
To the younger doctors on #MedTwitter: Take things slowly. Play your career like Test cricket, not T20.
Enjoy the little moments of life. Watch the sunset. Breathe mountain air. Cry with your friends. Read good fiction. Climb a rock. Fall in love.
Health and peace first. Everything else comes next. ✌️
🇬🇧 Famous British comedian Rowan Atkinson said:
“I feel ashamed on behalf of the United Kingdom for allowing Israel to besiege two million people in Gaza, cutting off their electricity, water, and medicine, and then claiming to defend human rights.”
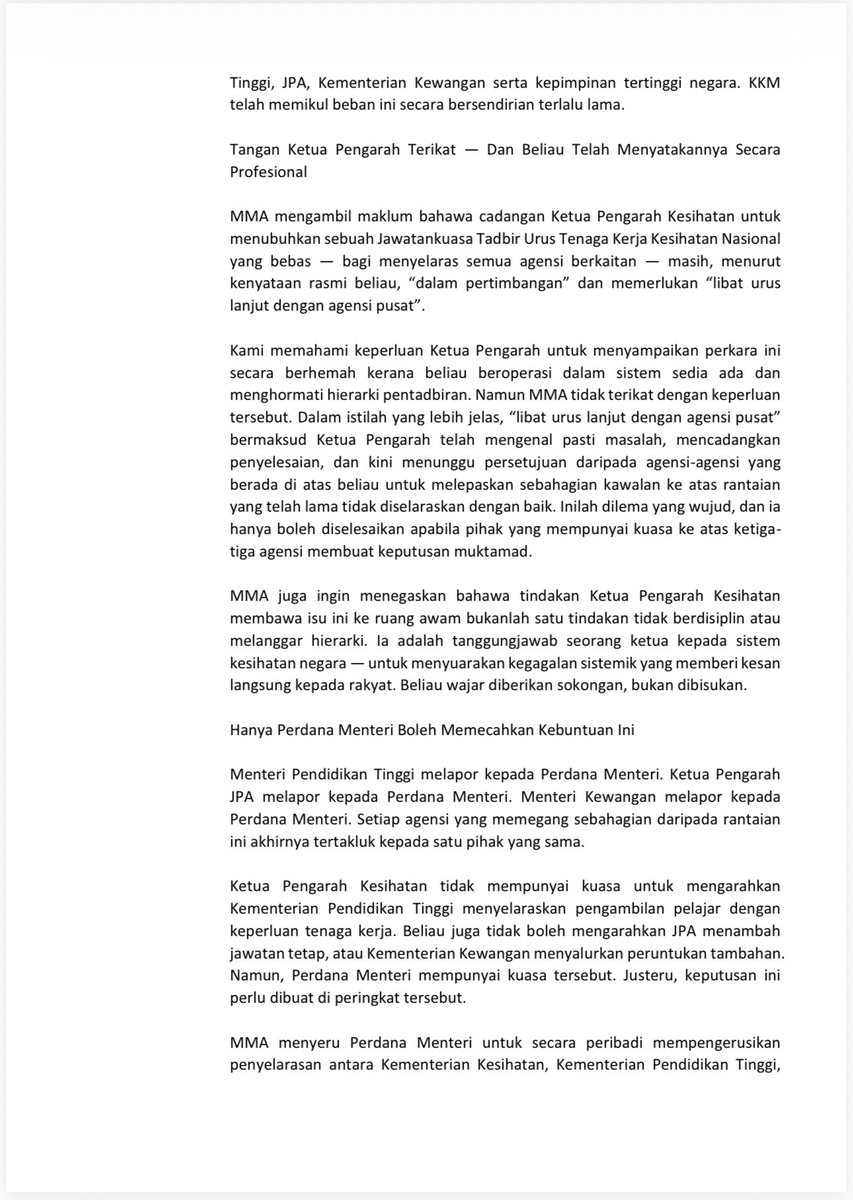
Penyelesaiannya jelas — Suruhanjaya Perkhidmatan Kesihatan dengan PEMBIAYAAN dan AUTORITI PENJAWATAN TERSENDIRI. KKM menyampaikan penjagaan — tetapi JPA, KPT dan MOF masing-masing memegang kunci. Hanya SATU individu berada di atas semua ini. YAB PMX @anwaribrahim — inilah saat itu. Kepada @MYParlimen — apabila bersidang Jun ini, jadikan ini agenda utama. Bukan demi kita. Demi 70% yang tiada pilihan lain. Pesakit kita tidak mampu menunggu. 👇📄
Akibatnya/The consequences:
• Doktor ada tapi tak dapat diserap
• Hospital kekurangan staf
• Doktor overworked
• Pesakit tunggu lebih lama
Hujung-hujung, patients pay the price.
Ini bukan kegagalan individu.
Ini kegagalan kepimpinan dan tadbir urus.
Pengambilan pelajar oleh MOHE.
Penjawatan oleh JPA.
Peruntukan oleh MOF.
Hospital dijalankan oleh MOH.
➡️ Semua bergerak sendiri.
Student intake → MOHE
Jobs/posts → JPA
Funding → MOF
Service delivery → MOH
➡️ No single command. No alignment.
DG KKM dah jelaskan.
Masalah sistem kesihatan kita bukan kekurangan doktor.
Masalah sebenar: sistem yang berpecah dan tak selaras.
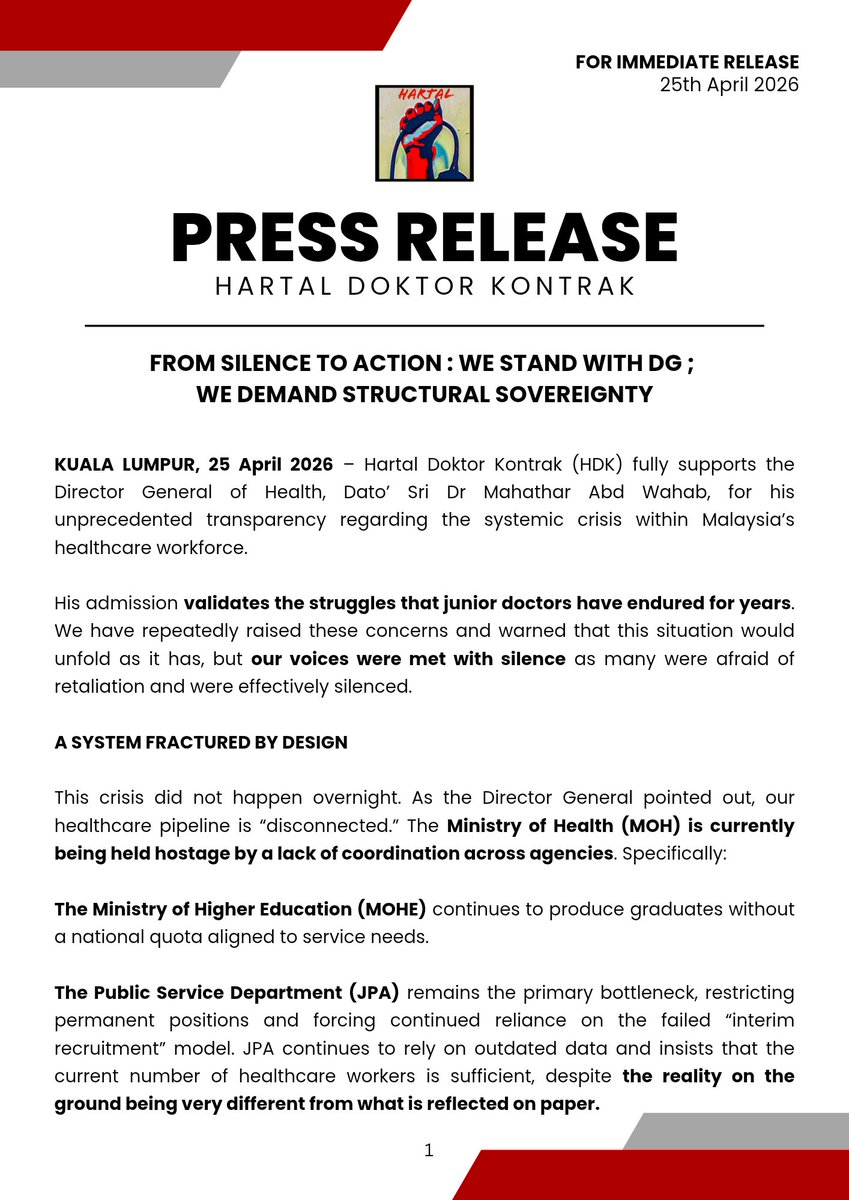
The Health DG has made it clear.
This is NOT a doctor shortage issue.
This is a system failure.
https://t.co/x8tm4yMY29
before the govt talks about AI, fix basic things like IT systems in our public hospitals first.
how can Ampang Hospital, Malaysia’s first paperless hospital, still be using a 20-year-old system and Windows XP???
why didn’t Putrajaya allocate the funds for crucial updates?
DG Mahathar says the doctor workforce pipeline is fragmented across MOHE, JPA, and MOH, causing delays and staff shortages despite adequate workforce numbers. He wants end-to-end workforce planning, competency-based approaches, and less “regulatory drag”.
https://t.co/raz2BdKdOF
NKF Malaysia chairman Dr Zaki Morad is frank about the impact of potential shortages of plastic-based dialysis medical devices and consumables due to the Persian Gulf conflict, saying all forms of kidney replacement therapy will be affected if supply chains are disrupted.
If shortages grow acute, he suggests reducing the frequency of dialysis treatment for suitable patients, optimising the strength of dialysate concentrate, or delaying the start of haemodialysis (HD) or peritoneal dialysis (PD) for new patients, with prolonged conservative treatment and close monitoring of affected patients instead.
"We do not stockpile dialysers or other consumables beyond two weeks’ usage as store space in our HD centres (and this is true for all HD centres) is very limited and these items are fast-moving," says Dr Zaki.
NKF, which treats some 1,800 patients in its 32 HD centres, isn't currently experiencing shortages of dialysers or other consumables.
Maaedicare Charitable Foundation, which has 11 dialysis centres, says it has a month's worth of buffer stock of dialysers and other HD consumables.
Socso, which operates 6 dialysis centres, says its centres maintain a "reasonable level of buffer stock based on usage patterns", boosted by a satellite stock arrangement.
Both Maaedicare and NKF aren't experiencing supply disruptions at the moment.
Dr Rosnawati Yahya, former head of the National Kidney Transplant Centre, urges MOH to form a nephrology task force to tackle dialysis product shortages as a national problem.
"We must prioritise central coordination over a fragmented response. Activating a central command structure at the MOH or network level and establishing a real-time stock visibility dashboard is essential to ensure equitable resource allocation and controlled distribution across all facilities, regardless of size," says Dr Rosnawati, a consultant nephrologist and kidney transplant physician at Sunway Medical Centre.
Read more: https://t.co/OAXcFo8C9t
A psychologist visits an engineer in his hospital bed...
The guy had just jumped off a bridge.
The psychologist says, "Hey there Ahmed, I'm Dr. Adams, how you feeling today?" And the engineer replies, "In pain, but lucky to be alive, I guess."
Dr. Adams wants to help, so she asks the engineer about his life. The engineer tells her he came from Libya a year ago. Life in Libya was rough, especially after Gaddafi was out. He told her about the power outages in Tripoli and studying electrical engineering by candlelight.
He finally got good enough to get a job in America. So he kisses his girlfriend goodbye, tells his family not to worry about food anymore—he'll start sending his paychecks home—and hops on a plane to California.
He's working 100-hour weeks at a startup called TechWave. Believes fully in the company. Even puts all his money into the company's stock.
The psychologist, she's heard of TechWave, thought they were doing great.
Asks him, "But TechWave is the new hot thing, why did you jump?"
"I thought they were too, but this morning I got a text saying the company would be closed for good Friday."
Tbt…at 15.59 Dr Bee Boon Cheak, Consultant Nephrologist alerted me with this short message..
Hi YB Datuk Seri,
Our deceased organ donor this morning, Selayang Hospital (liver, bilateral kidneys, bilateral corneas, heart and heart valve)..
He later gave a longer whasap and l take liberty to share it here…🙏
This is the story for this kindhearted young donor whose compassion touched everyone around him.
Just one month ago, he spoke to his parents about his wish to become an organ donor. With full understanding and love, they supported his decision.
According to his mother, he did not buy any Raya clothes this year — almost as if, deep down, he knew his time in this world would be short. On his phone, he had kept information about the National Kidney Foundation, a quiet reflection of his intention to give life to others.
Today, on what is also his mother’s birthday, she holds onto his final wish. Through her grief, she finds strength in honoring what he wanted — to give hope and life to others even after he is gone.🌹
With a mother’s love and courage, she pleaded with us to help fulfill her son’s last wish in this life.🥹
At around 4 a.m. this morning, the “walk of honor” took place. In those solemn moments, he was not alone. Surrounded by family and many friends, they walked alongside him — a final journey filled with love, respect, and gratitude.❤️
Though his life was brief, his legacy will live on in the lives he saves.🤲🤲🌺🌺😍😍
Tears welled in my eyes as l wrote back…
Dear Dr Bee,
In a moment of loss, this family chose courage, generosity, and humanity beyond measure. Their decision transforms grief into grace, and sorrow into salvation for others..❤️🌹
May God Almighty envelop this soul in His infinite Mercy-Rahmah, grant them the highest place in His Paradise & place them among those who are received with honour and tranquillity..🤲🌹❤️🤲
Every time you get a cancer biopsy, the lab makes a tissue slide that costs about $5. It shows the shape of your cells under a microscope, and every cancer patient already has one on file.
There’s a much fancier version of that test called multiplex immunofluorescence (basically a protein-level map showing which immune cells are near your tumor and what they’re doing). It costs thousands of dollars per sample, takes specialized equipment most hospitals don’t have, and barely scales. But it’s the kind of data oncologists need to figure out whether immunotherapy will actually work for you. Right now, only about 20 to 40% of cancer patients respond to immunotherapy, and one of the biggest reasons is that doctors can’t easily tell whether a tumor is “hot” (immune cells actively fighting it) or “cold” (immune system ignoring it).
Microsoft, Providence Health, and the University of Washington trained an AI to analyze the $5 slide and predict what the expensive test would show across 21 different protein markers. They called it GigaTIME, trained it on 40 million cells in which both the cheap slide and the expensive test coexisted, and then turned it loose on 14,256 real cancer patients across 51 hospitals in 7 US states.
The results landed in Cell, one of the most selective journals in biology. The model generated about 300,000 virtual protein maps covering 24 cancer types and 306 subtypes. It found 1,234 real, verified connections between immune cell behavior, genetic mutations, tumor staging, and patient survival that were previously invisible at this scale. When they tested it against a completely separate database of 10,200 cancer patients, the results matched up almost perfectly (0.88 out of 1.0 agreement).
Nature Methods named spatial proteomics (mapping where specific proteins sit inside your tissue) its Method of the Year in 2024, and specifically cited GigaTIME in a March 2026 update as a model that “democratizes” this kind of analysis. The full model is open-source on Hugging Face. Any cancer research lab with archived biopsy slides, and most of them have thousands, can now run virtual immune profiling without buying a single piece of new equipment.
this is actually insane
> be tech guy in australia
> adopt cancer riddled rescue dog, months to live
> not_going_to_give_you_up.mp4
> pay $3,000 to sequence her tumor DNA
> feed it to ChatGPT and AlphaFold
> zero background in biology
> identify mutated proteins, match them to drug targets
> design a custom mRNA cancer vaccine from scratch
> genomics professor is “gobsmacked” that some puppy lover did this on his own
> need ethics approval to administer it
> red tape takes longer than designing the vaccine
> 3 months, finally approved
> drive 10 hours to get rosie her first injection
> tumor halves
> coat gets glossy again
> dog is alive and happy
> professor: “if we can do this for a dog, why aren’t we rolling this out to humans?”
one man with a chatbot, and $3,000 just outperformed the entire pharmaceutical discovery pipeline.
we are going to cure so many diseases.
I dont think people realize how good things are going to get